Single-port plus an additional port robotic complete mesocolic excision and intracorporeal anastomosis using a robotic stapler for right-sided colon cancer
- Affiliations
-
- 1Department of Surgery, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, and Institute for Cancer Research, Daegu, Korea. sgbeak@dsmc.or.kr
- KMID: 2354330
- DOI: http://doi.org/10.4174/astr.2016.91.4.212
Abstract
- The concept of complete mesocolic excision and central vascular ligation for colonic cancer has been recently introduced. The paper describes a technique of right-sided complete mesocolic excision and intracorporeal anastomosis by using a single-port robotic approach with an additional conventional robotic port. We performed a single-port plus an additional port robotic surgery using the Da Vinci Single-Site platform via the Pfannenstiel incision and the wristed robotic instruments via an additional robotic port in the left lower quadrant. The total operative and docking times were 280 and 25 minutes, respectively. The total number of lymph nodes harvested was 36 and the proximal and distal resection margins were 31 and 50 cm, respectively. Single-port plus an additional port robotic surgery for right-sided complete mesocolic excision and intracorporeal anastomosis appears to be feasible and safe. This system can overcome certain limitations of the previous robotic systems and conventional single-port laparoscopic surgery.
MeSH Terms
Figure
-
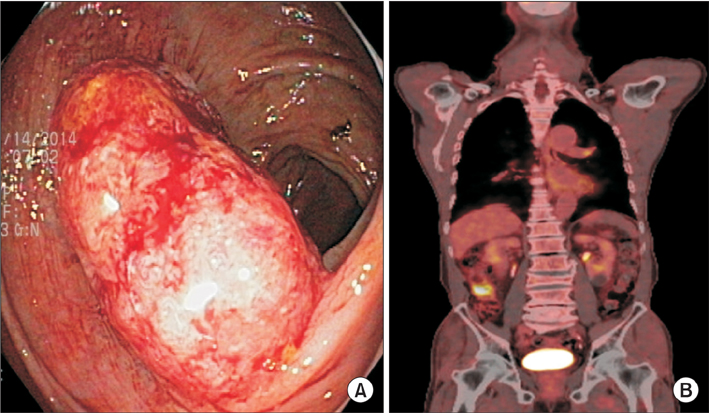
Fig. 1 (A) Colonoscopy reveals a 2-cm-sized ulcerofungating mass in the cecum, and (B) fluorodeoxyglucose scan reveals the hypermetabolic nature of the lesion.
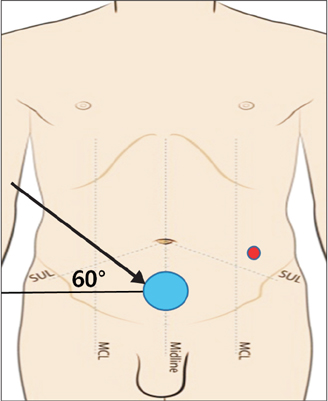
Fig. 2 Robotic cart placement and docking of the robotic ports. SUL, spino-umbilical line; MCL, midclavicular line.

Fig. 3 Adjustment of remote centers to secure the surgical space; (A) remote centers of R1, R2 cannulas and camera port are lifted upward out of the abdominal wall, and (B) all 3 remote centers are aligned at the same level.

Fig. 4 Access port setup for single-port plus an additional port robotic surgery for right-sided colon cancer.
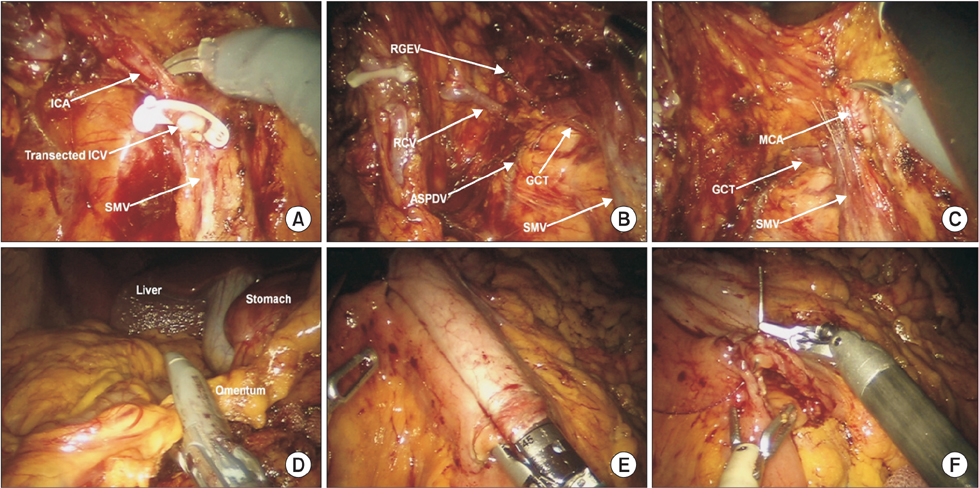
Fig. 5 Single-port plus an additional port robotic complete mesocolic excision with intracorporeal anastomosis, (A) Control of the ileocolic vessels, (B) colonic, pancreatic, and gastric branches draining to the gastrocolic trunk, (C) dissection around middle colic artery, (D) omental detachment for hepatic flexure mobilization using, (E) side-to-side intracorporeal isoperistaltic anastomosis with robotic stapler, and (F) closure of the stapler insertion site with robotic-assisted continuous stitches. ICA, ileocolic artery; ICV, ileocolic vein; SMV, superior mesenteric vein; RGEV, right gastroepiploic vein; RCV, right colic vein; ASPDV, anterior superior pancreaticoduodenal vein; GCT, gastrocolic trunk, MCA, middle colic artery

Fig. 6 The postoperative patient view. The additional port site is used for drain placement.
Cited by 1 articles
-
Learning curve for single-port robot-assisted rectal cancer surgery
Moon Suk Choi, Seong Hyeon Yun, Chang Kyu Oh, Jung Kyong Shin, Yoon Ah Park, Jung Wook Huh, Yong Beom Cho, Hee Cheol Kim, Woo Yong Lee
Ann Surg Treat Res. 2022;102(3):159-166. doi: 10.4174/astr.2022.102.3.159.
Reference
-
1. Nelson H, Petrelli N, Carlin A, Couture J, Fleshman J, Guillem J, et al. Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst. 2001; 93:583–596.2. Martling A, Holm T, Rutqvist LE, Johansson H, Moran BJ, Heald RJ, et al. Impact of a surgical training programme on rectal cancer outcomes in Stockholm. Br J Surg. 2005; 92:225–229.3. Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation--technical notes and outcome. Colorectal Dis. 2009; 11:354–364.4. Angus AA, Sahi SL, McIntosh BB. Learning curve and early clinical outcomes for a robotic surgery novice performing robotic single site cholecystectomy. Int J Med Robot. 2014; 10:203–207.5. Sendag F, Akdemir A, Zeybek B, Ozdemir A, Gunusen I, Oztekin MK. Single-site robotic total hysterectomy: standardization of technique and surgical outcomes. J Minim Invasive Gynecol. 2014; 21:689–694.6. Morelli L, Guadagni S, Caprili G, Di Candio G, Boggi U, Mosca F. Robotic right colectomy using the Da Vinci Single-Site® platform: case report. Int J Med Robot. 2013; 9:258–261.7. Spinoglio G, Lenti LM, Ravazzoni F, Formisano G, Pagliardi F, Marano A. Evaluation of technical feasibility and safety of Single-Site™ robotic right colectomy: three case reports. Int J Med Robot. 2015; 11:135–140.8. Bae SU, Jeong WK, Bae OS, Baek SK. Reduced-port robotic anterior resection for left-sided colon cancer using the Da Vinci single-site® platform. Int J Med Robot. 2015; 06. 23. [Epub]. DOI: 10.1002/rcs.1677.9. Bergamaschi R, Schochet E, Haughn C, Burke M, Reed JF 3rd, Arnaud JP. Standardized laparoscopic intracorporeal right colectomy for cancer: short-term outcome in 111 unselected patients. Dis Colon Rectum. 2008; 51:1350–1355.10. Hellan M, Anderson C, Pigazzi A. Extracorporeal versus intracorporeal anastomosis for laparoscopic right hemicolectomy. JSLS. 2009; 13:312–317.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intracorporeal Esophagojejunostomy during Reduced-port Totally Robotic Gastrectomy for Proximal Gastric Cancer: a Novel Application of the Single-Site ® Plus 2-port System
- Robotic versus laparoscopic surgery in colon and rectal cancer
- Robotic surgery for colorectal disease: review of current port placement and future perspectives
- Trocar Site Hernia after Use of an 8-mm Bladeless Trocar in Robotic Colorectal Surgery
- Feasibility and Potential of Reduced Port Surgery for Total Gastrectomy With Overlap Esophagojejunal Anastomosis Method
