Normal Caloric Responses during Acute Phase of Vestibular Neuritis
- Affiliations
-
- 1Department of Neurology, Ajou University School of Medicine, Ajou University Hospital, Suwon, Korea.
- 2Department of Neurology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. jisookim@snu.ac.kr
- 3Department of Biomedical Laboratory Science, Kyungdong University, Goseong, Korea.
- 4Department of Otolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2354117
- DOI: http://doi.org/10.3988/jcn.2016.12.3.301
Abstract
- BACKGROUND AND PURPOSE
We report a novel finding of caloric conversion from normal responses into unilateral paresis during the acute phase of vestibular neuritis (VN).
METHODS
We recruited 893 patients with a diagnosis of VN at Dizziness Clinic of Seoul National University Bundang Hospital from 2003 to 2014 after excluding 28 patients with isolated inferior divisional VN (n=14) and those without follow-up tests despite normal caloric responses initially (n=14). We retrospectively analyzed the neurotological findings in four (0.5%) of the patients who showed a conversion from initially normal caloric responses into unilateral paresis during the acute phase.
RESULTS
In those four patients, the initial caloric tests were performed within 2 days of symptom onset, and conversion into unilateral caloric paresis was documented 1-4 days later. The clinical and laboratory findings during the initial evaluation were consistent with VN in all four patients except for normal findings in bedside head impulse tests in one of them.
CONCLUSIONS
Normal findings in caloric tests should be interpreted with caution during the acute phase of suspected VN. Follow-up evaluation should be considered when the findings of the initial caloric test are normal, but VN remains the most plausible diagnosis.
MeSH Terms
Figure
-
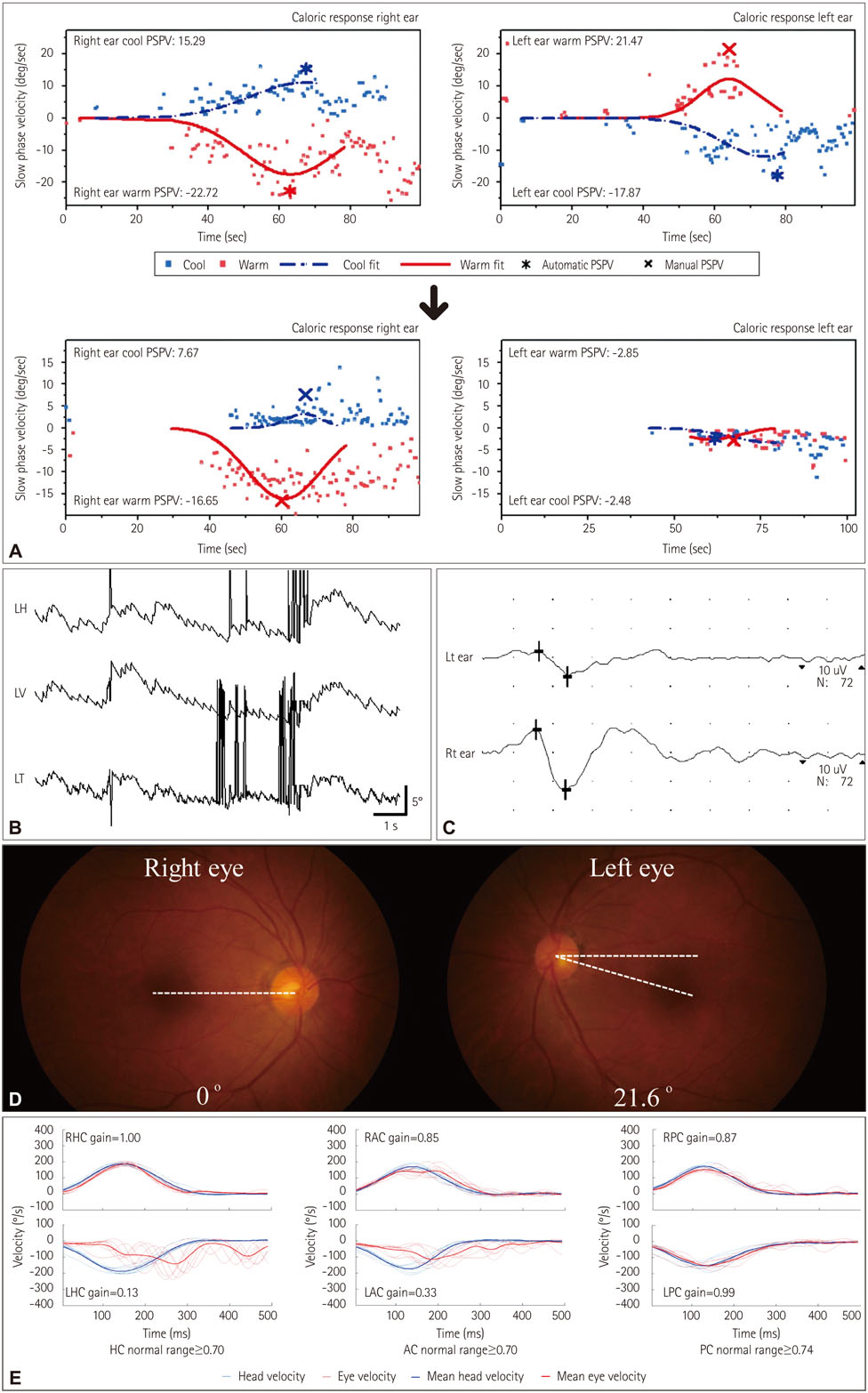
Fig. 1 Neurotological findings in patient 1. A: The initially normal caloric responses changed into complete left paralysis 4 days later. B: Video-oculography shows spontaneous nystagmus (SN) beating rightward, upward, and clockwise (from the patient's perspective). C: Ocular vestibular evoked myogenic potentials were decreased during left-ear stimulation. LH: horizontal position of the left eye, LV: vertical position of the left eye, LT: torsional position of the left eye, PSPV: peak slow-phase velocity. D: Fundus photography shows extorsion of the left eye (normal range: 0–12.6°, positive value indicates extorsion). E: Magnetic search coil recordings of head impulse tests show decreased gains for the left horizontal (HCs) and anterior canals (ACs), but normal gains for other semicircular canals including the left posterior canal (PC). LAC: left AC, LHC: left HC, LPC: left PC, RAC: right AC, RHC: right HC, RPC: right PC.

Fig. 2 Evolution of the bedside and laboratory neurotological findings in each patient. *Day 0: the day of symptom onset, †Evaluations using a magnetic search coil (MSC) technique. cVEMP: cervical vestibular-evoked myogenic potential, HIT: head-impulse test, HSN: head-shaking nystagmus, oVEMP: ocular vestibular-evoked myogenic potential, SN: spontaneous nystagmus, SVV: subjective visual vertical, VIN: vibration-induced nystagmus.
Reference
-
1. Jeong SH, Kim HJ, Kim JS. Vestibular neuritis. Semin Neurol. 2013; 33:185–194.
Article2. Strupp M, Brandt T. Vestibular neuritis. Semin Neurol. 2009; 29:509–519.
Article3. Baloh RW. Clinical practice. Vestibular neuritis. N Engl J Med. 2003; 348:1027–1032.4. Cnyrim CD, Newman-Toker D, Karch C, Brandt T, Strupp M. Bedside differentiation of vestibular neuritis from central "vestibular pseudoneuritis". J Neurol Neurosurg Psychiatry. 2008; 79:458–460.
Article5. Kim JS, Kim HJ. Inferior vestibular neuritis. J Neurol. 2012; 259:1553–1560.
Article6. Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol. 1988; 45:737–739.
Article7. Choi KD, Oh SY, Park SH, Kim JH, Koo JW, Kim JS. Head-shaking nystagmus in lateral medullary infarction: patterns and possible mechanisms. Neurology. 2007; 68:1337–1344.
Article8. Choi KD, Oh SY, Kim HJ, Kim JS. The vestibulo-ocular reflexes during head impulse in Wernicke's encephalopathy. J Neurol Neurosurg Psychiatry. 2007; 78:1161–1162.
Article9. Chen L, Todd M, Halmagyi GM, Aw S. Head impulse gain and saccade analysis in pontine-cerebellar stroke and vestibular neuritis. Neurology. 2014; 83:1513–1522.
Article10. Lehnen N, Aw ST, Todd MJ, Halmagyi GM. Head impulse test reveals residual semicircular canal function after vestibular neurectomy. Neurology. 2004; 62:2294–2296.
Article11. Kim HJ, Park SH, Kim JS, Koo JW, Kim CY, Kim YH, et al. Bilaterally abnormal head impulse tests indicate a large cerebellopontine angle tumor. J Clin Neurol. 2016; 12:65–74.
Article12. Choi KD, Oh SY, Kim HJ, Koo JW, Cho BM, Kim JS. Recovery of vestibular imbalances after vestibular neuritis. Laryngoscope. 2007; 117:1307–1312.
Article13. Kim S, Lee HS, Kim JS. Medial vestibulospinal tract lesions impair sacculo-collic reflexes. J Neurol. 2010; 257:825–832.
Article14. Baloh RW, Kerber KA, Honrubia V. Clinical Neurophysiology of the Vestibular System. 4th ed. New York, NY: Oxford University Press;2011.15. Maire R, van Melle G. Vestibulo-ocular reflex characteristics in patients with unilateral Ménière's disease. Otol Neurotol. 2008; 29:693–698.
Article16. Nadol JB Jr. Vestibular neuritis. Otolaryngol Head Neck Surg. 1995; 112:162–172.17. Schuknecht HF, Kitamura K. Second Louis H. Clerf Lecture. Vestibular neuritis. Ann Otol Rhinol Laryngol Suppl. 1981; 90(1 Pt 2):1–19.18. Schmid-Priscoveanu A, Böhmer A, Obzina H, Straumann D. Caloric and search-coil head-impulse testing in patients after vestibular neuritis. J Assoc Res Otolaryngol. 2001; 2:72–78.
Article19. Lee H, Kim BK, Park HJ, Koo JW, Kim JS. Prodromal dizziness in vestibular neuritis: frequency and clinical implication. J Neurol Neurosurg Psychiatry. 2009; 80:355–356.
Article20. Proctor L, Glackin R. Factors contributing to variability of caloric test scores. Acta Otolaryngol. 1985; 100:161–171.
Article21. Baertschi AJ, Johnson RN, Hanna GR. A theoretical and experimental determination of vestibular dynamics in caloric stimulation. Biol Cybern. 1975; 20:175–186.
Article22. Furman JM, Jacob RG. Jongkees' formula re-evaluated: order effects in the response to alternate binaural bithermal caloric stimulation using closed-loop irrigation. Acta Otolaryngol. 1993; 113:3–10.
Article23. Lee H, Sohn SI, Cho YW, Lee SR, Ahn BH, Park BR, et al. Cerebellar infarction presenting isolated vertigo: frequency and vascular topographical patterns. Neurology. 2006; 67:1178–1183.
Article24. Kim JS, Lee H. Vertigo due to posterior circulation stroke. Semin Neurol. 2013; 33:179–184.
Article25. Jorns-Häderli M, Straumann D, Palla A. Accuracy of the bedside head impulse test in detecting vestibular hypofunction. J Neurol Neurosurg Psychiatry. 2007; 78:1113–1118.
Article26. Lee H, Kim JS, Chung EJ, Yi HA, Chung IS, Lee SR, et al. Infarction in the territory of anterior inferior cerebellar artery: spectrum of audiovestibular loss. Stroke. 2009; 40:3745–3751.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Inferior Vestibular Neuritis: Absence of Vestibular Evoked Myogenic Potentials in the Presence of Normal Caloric Responses
- Follow-up Changes of Eye Movements by Caloric Stimulation in Patients With Vestibular Neuritis
- Cervical Vestibular Evoked Myogenic Potential and Ocular Vestibular Evoked Myogenic Potential in Patients With Vestibular Neuritis and Acute Viral Labyrinthitis
- A Case of Selective Inferior Vestibular Neuritis Showing Normal Caloric Test
- Long-Term Changes in Video Head Impulse and Caloric Tests in Patients with Unilateral Vestibular Neuritis
