Multifocal Extensive Spinal Tuberculosis Accompanying Isolated Involvement of Posterior Elements: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, CHA Bundang Medical Center, CHA University, Korea. ajh329@gmail.com
- KMID: 2353910
- DOI: http://doi.org/10.4184/jkss.2016.23.3.183
Abstract
- STUDY DESIGN: A case report.
OBJECTIVES
To report a rare case of atypical spinal tuberculosis. SUMMARY OF LITERATURE REVIEW: In spinal tuberculosis, non-contiguous multifocal involvement and isolated involvement of posterior elements of the spine have been considered atypical features. There have been a few reports of each of these atypical features but no reports have described spinal tuberculosis with both of these atypical features.
MATERIALS AND METHODS
A 39-year-old man presented with back pain and progressive weakness of both lower extremities. He was diagnosed with spinal tuberculosis from the cervical to sacral spine, showing multifocal non-contiguous involvement with multiple abscesses on magnetic resonance imaging. Notably, in the thoracic spine area, isolated involvement of posterior elements was found with an epidural abscess compressing the spinal cord. He underwent a total laminectomy of the thoracic spine and multiple abscesses were drained with pigtail catheter insertions into the cervical, thoracic, and lumbar spine.
RESULTS
At the 8-month follow-up, the patient's neurologic status had improved to Frankel Grade D, and the patient was able to walk with the support of a walker. At the 3-year follow-up, the patient had recovered completely without any neurologic deficit.
CONCLUSIONS
Since atypical spinal tuberculosis may show various patterns, examination of the entire spine is important for early diagnosis. Treatment should be provided properly from minimally invasive procedures to open surgery depending on the extent of structural instability and neurologic deficit.
Keyword
MeSH Terms
Figure
-
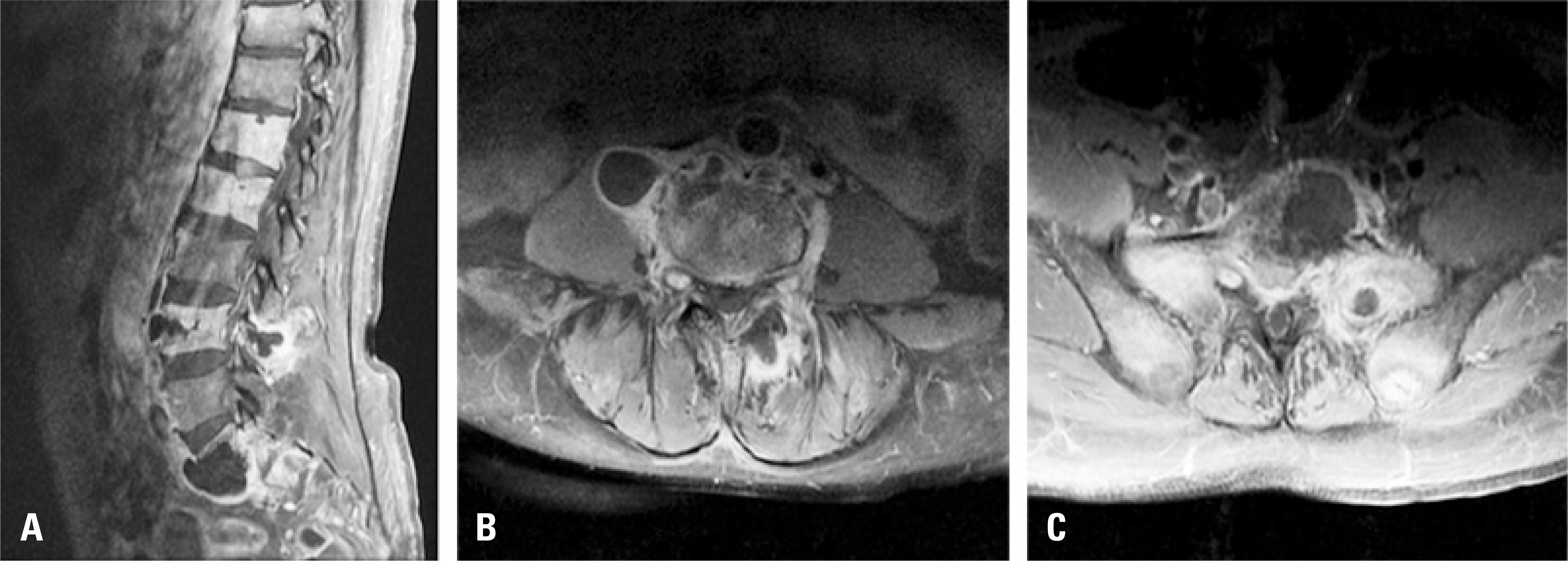
Fig. 1. Enhanced T1-weighted magnetic resonance images of the lumbosacral spine with fat suppression. (A) A sagittal image showing high signals at T11, L1, L2, L4, S1, and S2 with abscesses at the L4 and S1 levels. (B) Abscesses in the anterior vertebral body, right psoas muscle, and left erector muscle at the L4 level on an axial image. (C) Abscesses in the sacrum extending to the presacral space and high signals in the sacrum and both sacral ala.
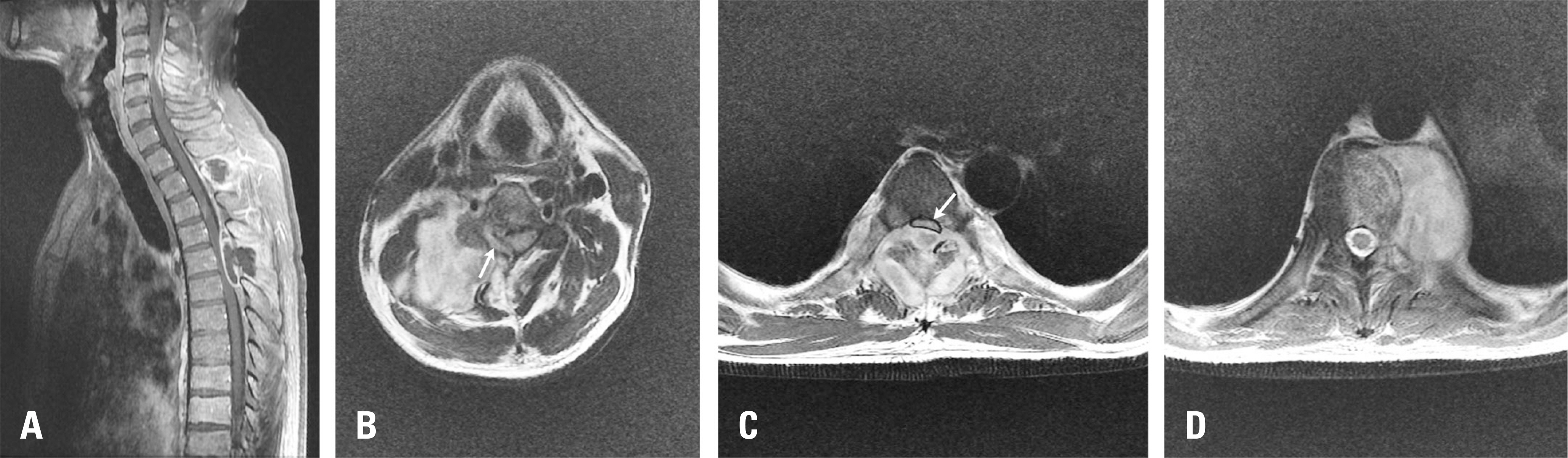
Fig. 2. Magnetic resonance images of the cervical and thoracic spine. (A) An enhanced sagittal T1-weighted image. In the cervical spine, the cord compressing the epidural abscess with high signals in the C4 vertebral body and posterior osteoligamentous structures of the C3-C5 levels was found. In the thoracic spine, two abscesses limited to the posterior elements of the T2 and T4-T6 levels were revealed. Notably, the posterior epidural abscess of the T4-T6 level was compressing the spinal cord, causing progressive neurologic deficits. (B) An axial T2-weighted image of the C4 level showing a huge right paravertebral abscess and spinal cord deviation to the right side by the right posterior epidural abscess (white arrow). (C) Severe cord compression (white arrow) by a huge posterior abscess involving the posterior epidural space and posterior elements on an axial T2-weighted image at the C5-C6 intervertebral disc level. (D) A left-sided anterior paravertebral abscess with involvement of the vertebral body, pedicle, and lamina at the T10 level on the axial T2-weighted image.
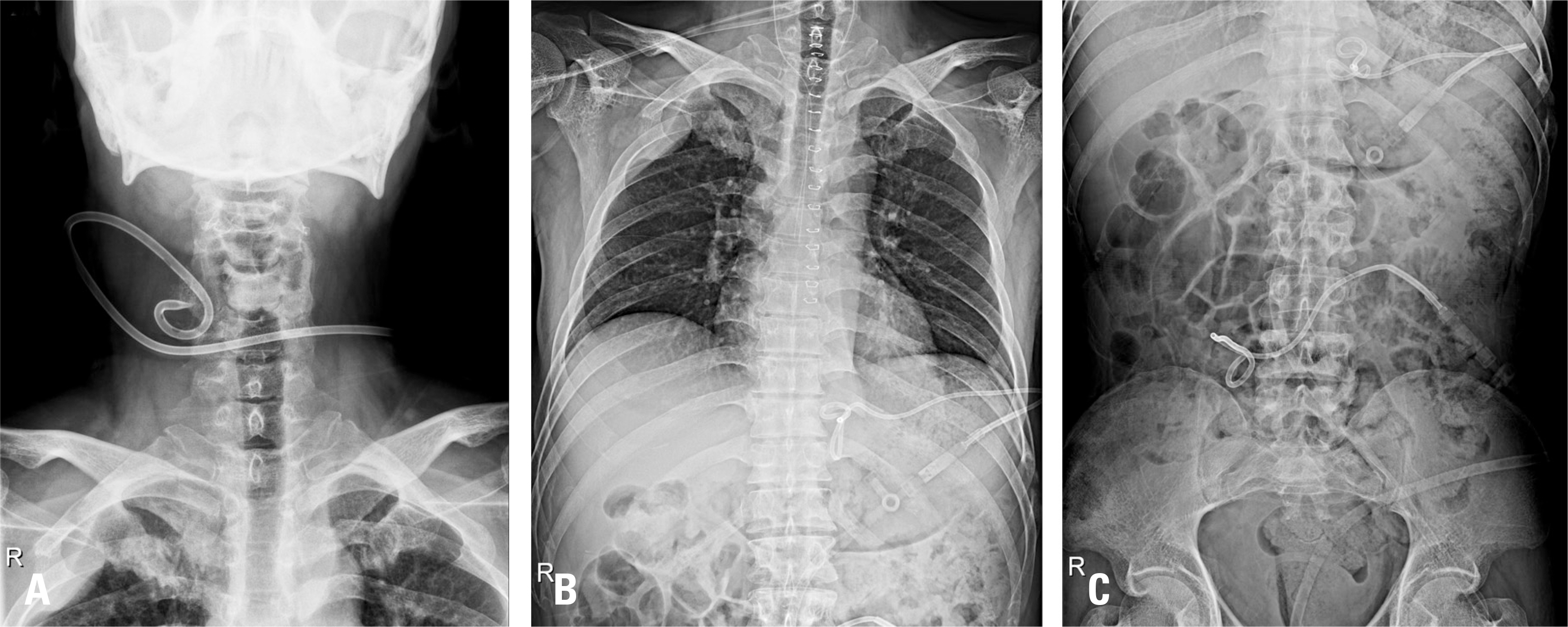
Fig. 3. Plain radiographs of the cervical, thoracic, and lumbosacral spine after pigtail catheter insertions. (A) Pigtail insertion into the right paravertebral area at C3 to C4. (B) Pigtail insertion into the left paravertebral area at T8 to T11. (C) Pigtail insertion into the right paravertebral area.
Reference
-
1. Harry N. Herkowitz, Steven R Garfin, Frank J. Eismont, et al. Rothman-Simeone the spine: expert consult. 6th ed.Elsevier Health Sciences:;2011. 1535.2. Lolge S, Maheshwari M, Shah J, et al. Isolated solitary vertebral body tuberculosis—study of seven cases. Clin Radiol. 2003; 58:545–50.
Article3. Wellons JC, Zomorodi AR, Villaviciencio AT, et al. Sacral tuberculosis: a case report and review of the literature. Surg Neurol. 2004; 61:136–9.
Article4. Al-Arabi KM, Khan FA. Atypical forms of spinal tuberculosis. Acta Neurochir (Wien). 1987; 88:26–33.5. Sankaran-Kutty M. Atypical tuberculous spondylitis. Int Orthop. 1992; 16:69–74.
Article6. Emel E, Gü zey FK, Gü zey D, et al. Non-contiguous multifocal spinal tuberculosis involving cervical, thoracic, lumbar and sacral segments: a case report. Eur Spine J. 2006; 15:1019–24.
Article7. Pieri S, Agresti P, Altieri AM, et al. Percutaneous management of complications of tuberculous spondylodiscitis: short-to medium-term results. Radiol Med. 2009; 114:984–95.8. Turgut M. Multifocal extensive spinal tuberculosis (Pott's disease) involving cervical, thoracic and lumbar vertebrae. Br J Neurosurg. 2001; 15:142–6.
Article9. Arora S, Sabat D, Maini L, et al. Isolated involvement of the posterior elements in spinal tuberculosis. J Bone Joint Surg Am. 2012; 94:E151.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multifocal Pott's Disease: A Report of Two Cases
- Tuberculous Epididymo-Orchitis with Multifocal Extrapulmonary Tuberculosis: a Case Report
- Atypical tuberculosis of the spine
- Atypical Form of Multiple Spinal Tuberculosis
- Atypical Presentation of Spinal Tuberculosis Misadiagnosed as Metastatic Spine Tumor
