Microdochectomy Assisted by Ultrasound-Guided Indigo Carmine Staining of Intraductal Lesions: A Case Report
- Affiliations
-
- 1Department of Radiology, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea. dbkim@dumc.or.kr
- 2Department of Surgery, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea.
Abstract
- Spontaneous bloody nipple discharge from a single duct is a significant clinical problem. When performing preoperative marking of the discharging duct, it is sometimes difficult to identify the duct owing to intermittent discharge. Precise preoperative marking of the discharging duct and intraductal lesions is very important to avoid unnecessary wide excision of breast tissue or failure to remove the cause of nipple discharge. We herein present a case of preoperative ultrasound-guided indigo carmine staining in a patient with no discharge on the day of surgery. When a dilated duct is visualized on ultrasound, the targeted duct can be localized using indigo carmine staining, and it is possible to perform a precise minimal volume microdochectomy.
Keyword
Figure
-
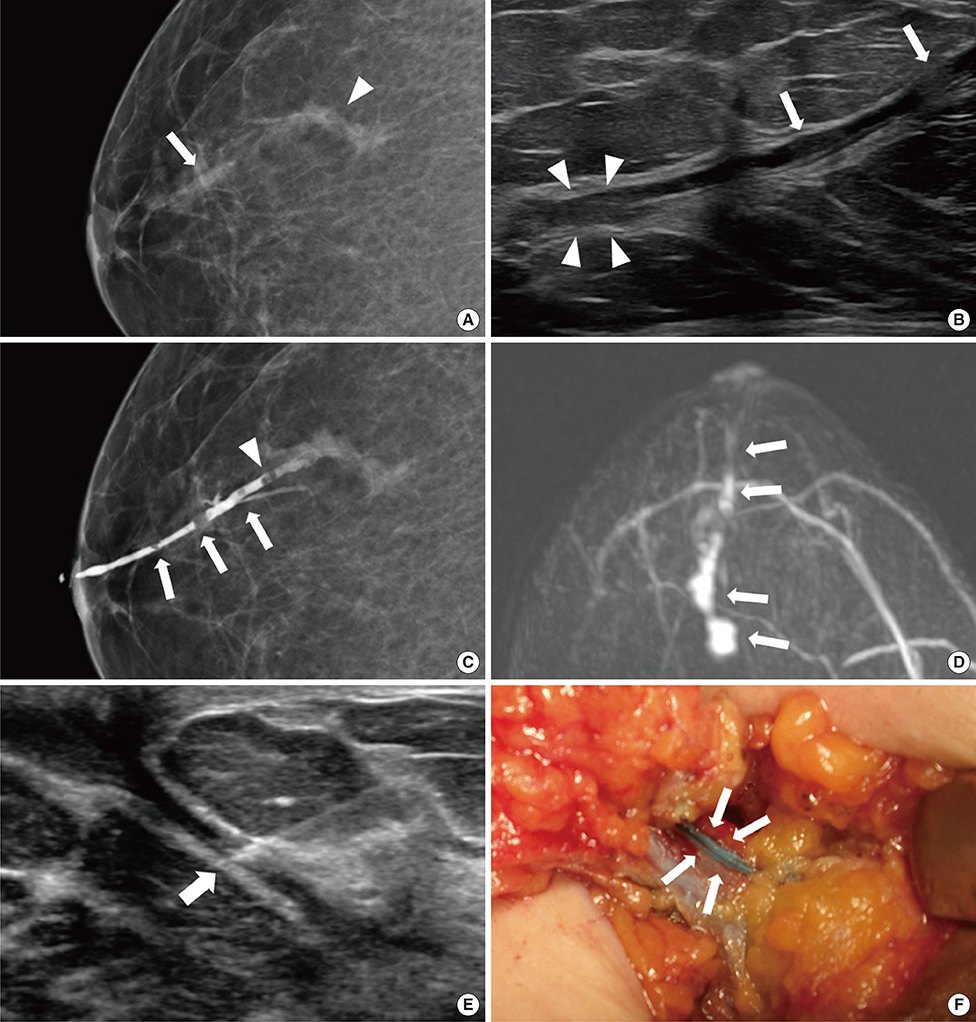
Figure 1 Images of a 35-year-old female with spontaneously intermittent bloody discharge from the right nipple for 4 months. (A) A mammography shows an asymmetric tubular structure in the subareolar area (arrow) and a 3.2 cm tortuous tubular structure (arrowhead) in the upper outer quadrant of the right breast. (B) A sonogram shows a dilated duct with isoechoic intraductal lesions (arrows) in the subareolar area and 2 cm from the nipple and a tortuous tubular intra- and extra-ductal mass (arrowheads) 5 cm from the nipple. (C) A right craniocaudal galactogram shows three polypoid filling defects (arrows) and ductal cutoff (arrowhead) in the dilated lactiferous duct. This dilated duct is correlated with the asymmetric tubular tortuous structures in the subareolar area and upper outer quadrant of the right breast on mammography (not shown). (D) The reconstructed maximum intensity projection of a contrast-enhanced magnetic resonance image shows a 4.4 cm area of linear and clumped nonmass enhancement (arrows). (E) On the day of the surgery, a needle (arrow) was inserted in the dilated duct in the 10 o'clock region of the right breast under ultrasound guidance. After injection of a small volume of indigo carmine into the dilated duct, the targeted duct became more dilated, and dye was discharged from the one orifice of the right nipple (not shown). (F) Photograph of the microdochectomy procedure. After dissection, the indigo carmine-stained duct (arrows) was evident in the operative field, and was easy to perform minimal-volume microdochectomy.
Reference
-
1. Saarela AO, Kiviniemi HO, Rissanen TJ. Preoperative methylene blue staining of galactographically suspicious breast lesions. Int Surg. 1997; 82:403–405.2. Hahn M, Fehm T, Solomayer EF, Siegmann KC, Hengstmann AS, Wallwiener D, et al. Selective microdochectomy after ductoscopic wire marking in women with pathological nipple discharge. BMC Cancer. 2009; 9:151.
Article3. Ferris-James DM, Iuanow E, Mehta TS, Shaheen RM, Slanetz PJ. Imaging approaches to diagnosis and management of common ductal abnormalities. Radiographics. 2012; 32:1009–1030.
Article4. Rissanen T, Reinikainen H, Apaja-Sarkkinen M. Breast sonography in localizing the cause of nipple discharge: comparison with galactography in 52 patients. J Ultrasound Med. 2007; 26:1031–1039.5. Rissanen T, Typpö T, Tikkakoski T, Turunen J, Myllymäki T, Suramo I. Ultrasound-guided percutaneous galactography. J Clin Ultrasound. 1993; 21:497–502.
Article6. Hussain S, Lui DM. Ultrasound guided percutaneous galactography. Eur J Radiol. 1997; 24:163–165.
Article7. Dinkel HP, Trusen A, Gassel AM, Rominger M, Lourens S, Müller T, et al. Predictive value of galactographic patterns for benign and malignant neoplasms of the breast in patients with nipple discharge. Br J Radiol. 2000; 73:706–714.
Article8. Koskela A, Berg M, Pietiläinen T, Mustonen P, Vanninen R. Breast lesions causing nipple discharge: preoperative galactography-aided stereotactic wire localization. AJR Am J Roentgenol. 2005; 184:1795–1798.
Article9. Sharma N, Huston TL, Simmons RM. Intraoperative intraductal injection of methylene blue dye to assist in major duct excision. Am J Surg. 2006; 191:553–554.
Article10. Dillon MF, Mohd Nazri SR, Nasir S, McDermott EW, Evoy D, Crotty TB, et al. The role of major duct excision and microdochectomy in the detection of breast carcinoma. BMC Cancer. 2006; 6:164.
Article11. Jo YY, Lee MG, Yun SY, Lee KC. Profound hypotension after an intradermal injection of indigo carmine for sentinel node mapping. J Breast Cancer. 2013; 16:127–128.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypotension in patients administered indigo carmine containing impurities: A case report
- Cardiac arrest from intravenous indigo carmine during laparoscopic surgery: A case report
- Detection of Polyps Including Adenomas in the Ascending Colon by Cap-assisted Chromocolonoscopy with Indigo Carmine
- Profound Hypotension after an Intradermal Injection of Indigo Carmine for Sentinel Node Mapping
- Extreme Hypotension Followed by an Intravenous Indigo Carmine Injection during a Radical Prostatectomy: A case report
