An Experimental Study for Minimum Level of Decalcification to Detect the Osteolytic Bone Metastasis of Long Bone on Plain Radiography
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kyungpook National University Hospital, Daegu, Korea. ihpark@knu.ac.kr
- 2Department of Medical and Health Science, Gyeongju University, Gyeongju, Korea.
- KMID: 2350809
- DOI: http://doi.org/10.11005/jbm.2016.23.3.135
Abstract
- BACKGROUND
In 1951, Ardran reported that metastatic bone lesions could be detectable on plain radiography with 30% to 50% of decalcification. Authors performed experimental study for minimum level of decalcification to detect the osteolytic bone metastasis of long bone with recent technique of radiographs.
METHODS
One pair of fibula and humerus from two cadavers was cut into specimen 1 inch in length. Distal half of specimen was dipped into hydrochloride (HCl) with 15 min interval. All 16 specimens were checked by film-type radiography (FR), computed radiography (CR), digital radiography (DR). To exclude inter-observer's variance, 3 radiologists evaluated images. Calcium amount before and after decalcification was measured and expressed in percentage of decalcification.
RESULTS
Osteolytic changes were detectable with 11% to 16% of decalcification for fibula and 3% to 8% for humerus on plain radiography with FR, CR, and DR.
CONCLUSIONS
Our study showed that minimum of 3% and maximum of 16% of decalcification is necessary when osteolytic metastatic bone lesions of long bone could be detected on plain radiography.
MeSH Terms
Figure
-
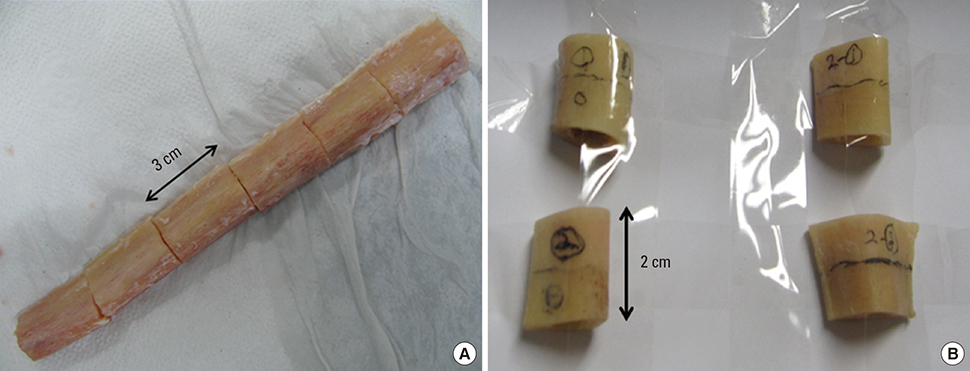
Fig. 1 (A) A cadaveric right fibula shaft was divided into 6 specimens with 3 cm in length. (B) A pair of cadaveric humeral shaft were divided into 10 specimens with 2 cm in length.
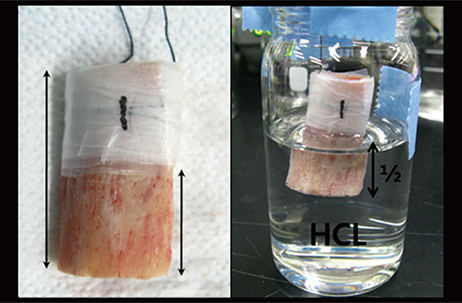
Fig. 2 Distal half of each specimen was immersed into 1 N HCl for decalcification process; 30, 60, 90, 120, 150, 180 min for fibula, 15, 30, 45, 60, 75 min for humerus. Non-decalcified area was covered by Parafilm.
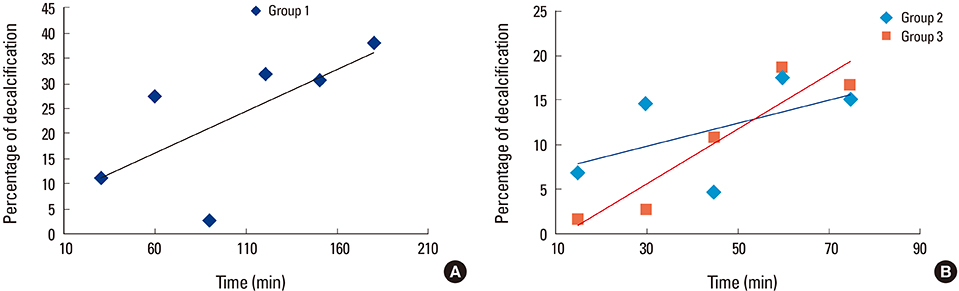
Fig. 3 (A) Rate (%) of decalcification with time (min) for group 1 (fibula). (B) Rate (%) of decalcification with time (min) for group 2, group 3 (humerus).

Fig. 4 (A) Serial radiographs of computed radiography showed gradual progression of decalcification with time (min) in fibula. (B) Serial radiographs of digital radiography showed gradual progression of decalcification with time (min) in fibula.
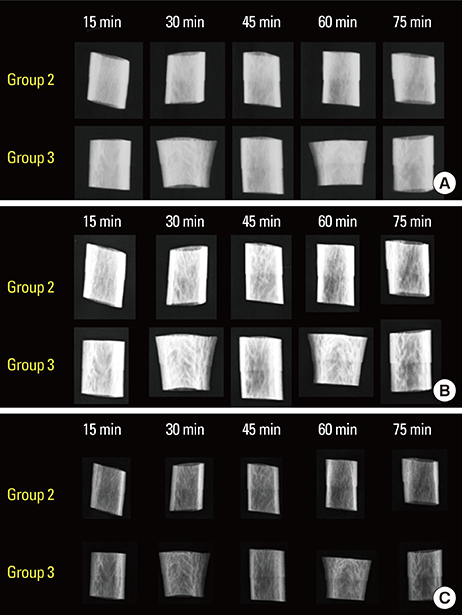
Fig. 5 (A) Serial radiographs of film-type radiography showed gradual progression of decalcification with time (min) in humerus. (B) Serial radiographs of computed radiography showed gradual progression of decalcification with time (min) in humerus. (C) Serial radiographs of digital radiography showed gradual progression of decalcification with time (min) in humerus.
Reference
-
1. McAdams HP, Samei E, Dobbins J 3rd, et al. Recent advances in chest radiography. Radiology. 2006; 241:663–683.
Article2. Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. 1950; 3:74–85.
Article3. Mundy GR. Mechanisms of bone metastasis. Cancer. 1997; 80:1546–1556.
Article4. Plunkett TA, Rubens RD. The biology and management of bone metastases. Crit Rev Oncol Hematol. 1999; 31:89–96.
Article5. Elgazzar AH, Kazem N. Metastatic bone disease: evaluation by functional imaging in correlation with morphologic modalities. Gulf J Oncolog. 2009; 9–21.6. Ghanem N, Uhl M, Brink I, et al. Diagnostic value of MRI in comparison to scintigraphy, PET, MS-CT and PET/CT for the detection of metastases of bone. Eur J Radiol. 2005; 55:41–55.
Article7. Ardran GM. Bone destruction not demonstrable by radiography. Br J Radiol. 1951; 24:107–109.
Article8. Nystrom JS, Weiner JM, Heffelfinger-Juttner J, et al. Metastatic and histologic presentations in unknown primary cancer. Semin Oncol. 1977; 4:53–58.9. Greenfield GB, Arrington JA. Imaging of bone tumors: a multimodality approach. Philadelphia, PA: Lippincott Williams & Wilkins;1995.10. Schaefer-Prokop CM, De Boo DW, Uffmann M, et al. DR and CR: Recent advances in technology. Eur J Radiol. 2009; 72:194–201.
Article11. Cowen AR, Davies AG, Kengyelics SM. Advances in computed radiography systems and their physical imaging characteristics. Clin Radiol. 2007; 62:1132–1141.
Article12. Gruber M, Uffmann M, Weber M, et al. Direct detector radiography versus dual reading computed radiography: feasibility of dose reduction in chest radiography. Eur Radiol. 2006; 16:1544–1550.
Article13. Neitzel U. Status and prospects of digital detector technology for CR and DR. Radiat Prot Dosimetry. 2005; 114:32–38.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Change of the fractal dimension according to the decalcification degree and the exposure time in the bovine rib
- The Value of Bone Scan for Detection of Bone Metastasis of Prostatic Cancer
- Multiple myeloma : 45 cases -plain X-ray and bone scan-
- Multicentric Primary Angiosarcoma of Bone Mimicking Metastasis on 18F-FDG PET/CT in a Patient with a History of Sigmoid Colon Cancer: a Case Report
- The Role of Whole Body Bone Scan in Bronchogenic Carcinoma
