Recurrent hyperparathyroidism due to proliferation of autotransplanted parathyroid tissue in a multiple endocrine neoplasia type 2A patient
- Affiliations
-
- 1Department of Surgery, Daejeon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. sun2729@naver.com
- KMID: 2350542
- DOI: http://doi.org/10.4174/astr.2016.91.3.145
Abstract
- About 20%-30% of all cases of multiple endocrine neoplasia type 2A (MEN 2A) is accompanied by primary hyperparathyroidism. These patients undergo parathyroidectomy and, if needed, autotransplantation. In rare cases, autotransplanted parathyroid tissues can cause hypoparathyroidism due to failure of transplantation or hyperparathyroidism due to proliferation of the transplanted tissue. A 68-year-old female with MEN 2A underwent left adrenalectomy for pheochromocytoma 15 years prior to presentation and total thyroidectomy, central and right lateral neck lymph node dissection, and subtotal parathyroidectomy with autotransplantation for medullary thyroid cancer and primary hyperparathyroidism 6 years previous. Recently, a doubtful parathyroid adenoma was detected in the left sternocleidomastoid muscle on ultrasonography and on an additional sestamibi scan. The mass was excised and histologically confirmed as parathyroid adenoma. This is a very rare case, and it suggests that long-term regular monitoring of serum calcium and intact parathyroid hormone levels is necessary after parathyroid autotransplantation.
Keyword
MeSH Terms
-
Adrenalectomy
Aged
Autografts
Calcium
Female
Humans
Hyperparathyroidism*
Hyperparathyroidism, Primary
Hypoparathyroidism
Lymph Node Excision
Multiple Endocrine Neoplasia Type 2a*
Multiple Endocrine Neoplasia*
Neck
Parathyroid Glands
Parathyroid Hormone
Parathyroid Neoplasms
Parathyroidectomy
Pheochromocytoma
Recurrence
Thyroid Neoplasms
Thyroidectomy
Transplantation, Autologous
Ultrasonography
Calcium
Parathyroid Hormone
Figure
-

Fig. 1 The patient's familial diagram. The patient (black arrow) and her siblings had all undergone thyroidectomy (filled with gray). Some of her siblings were diagnosed with medullary thyroid cancer.
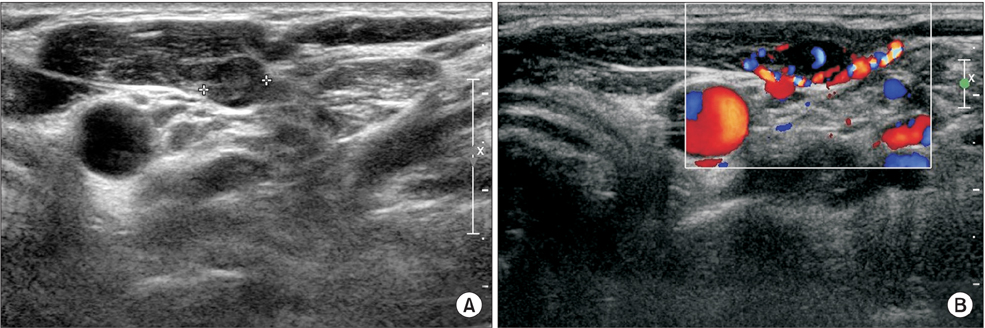
Fig. 2 Ultrasonographic image of a 68-year-old female with recurrent hyperparathyroidism. (A) A 1.3 cm × 0.6 cm round hypoechoic nodule in the left sternocleidomastoid muscle. (B) The nodule was well supplied with vessels according to Doppler flow mode.
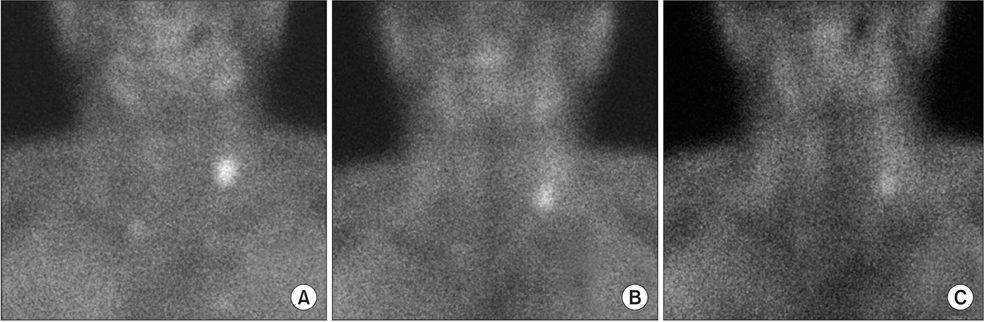
Fig. 3 A sestamibi scan. (A) 10 minutes, (B) 2 hours, and (C) 3 hours after administration, focal hot uptake was observed.
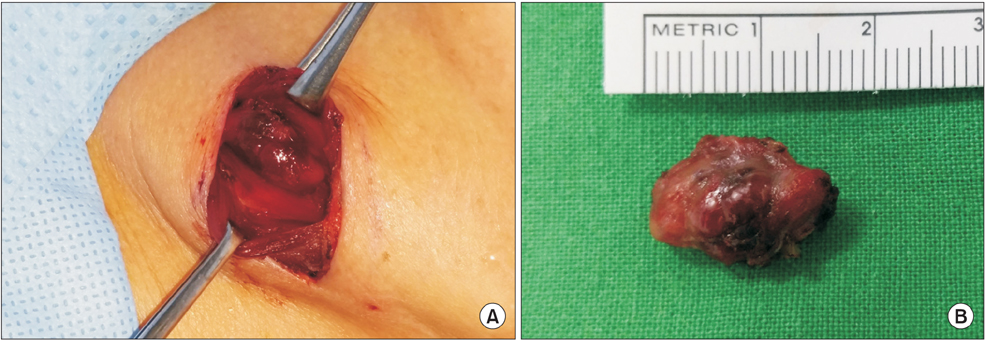
Fig. 4 (A) Parathyroid adenoma excision. A transplanted parathyroid adenoma in the sternal part of the left sternocleidomastoid muscle. (B) An excised parathyroid adenoma consisting of a 1.6-cm ovoid mass.
Reference
-
1. Taieb D, Kebebew E, Castinetti F, Chen CC, Henry JF, Pacak K. Diagnosis and preoperative imaging of multiple endocrine neoplasia type 2: current status and future directions. Clin Endocrinol (Oxf). 2014; 81:317–328.2. Carling T, Udelsman R. Parathyroid surgery in familial hyperparathyroid disorders. J Intern Med. 2005; 257:27–37.3. Park JH, Lee HK, Nam SJ, Jung JH, Lee MS, Yang JH. Multiple endocrine neoplasia type IIa report of three cases. J Korean Surg Soc. 2000; 59:115–123.4. Halsted WS. Auto- and isotransplantation, in dogs, of the parathyroid glandules. J Exp Med. 1909; 11:175–199.5. Senapati A, Young AE. Parathyroid autotransplantation. Br J Surg. 1990; 77:1171–1174.6. Yoshida S, Imai T, Kikumori T, Wada M, Sawaki M, Takada H, et al. Long term parathyroid function following total parathyroidectomy with autotransplantation in adult patients with MEN2A. Endocr J. 2009; 56:545–551.7. D'Avanzo A, Parangi S, Morita E, Duh QY, Siperstein AE, Clark OH. Hyperparathyroidism after thyroid surgery and autotransplantation of histologically normal parathyroid glands. J Am Coll Surg. 2000; 190:546–552.8. Mulligan LM, Eng C, Healey CS, Clayton D, Kwok JB, Gardner E, et al. Specific mutations of the RET proto-oncogene are related to disease phenotype in MEN 2A and FMTC. Nat Genet. 1994; 6:70–74.9. Hedback G, Oden A. Recurrence of hyperparathyroidism; a long-term follow-up after surgery for primary hyperparathyroidism. Eur J Endocrinol. 2003; 148:413–421.10. Cavallaro G, Iorio O, Centanni M, Porta N, Iossa A, Gargano L, et al. Parathyroid reimplantation in forearm subcutaneous tissue during thyroidectomy: a simple and effective way to avoid hypoparathyroidism. World J Surg. 2015; 39:1936–1942.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Endocrine Neoplasia 2A Detected by Peptic Ulcer Perforation with Hypercalcemia
- Multiple Endocrine Neoplasia and Familial Medullary Thyroid Carcinoma
- Ectopic ACTH Syndrome with Bilateral Pheochromocytoma in Multiple Endocrine Neoplasia Type 2A
- A Case of Asymptomatic Multiple Endocrine Neoplasia Type 1 Detected Incidentally on Health Screening
- A Case of Familial Multiple Endocrine Neoplasia with MEN1 Gene Mutation
