Chronological Endoscopic and Pathological Observations in Russell Body Duodenitis
- Affiliations
-
- 1Department of Gastroenterology and Hepatology, Yamaguchi University Graduate School of Medicine, Ube, Japan. gotomukku@yahoo.co.jp
- 2Department of Gastroenterology and Hepatology, Hagi Civil Hospital, Hagi, Japan.
- 3Department of General Medicine, Hagi Civil Hospital, Hagi, Japan.
- 4Department of Gastroenterology and Hepatology, Kanmon Medical Center, Shimonoseki, Japan.
- 5Department of Molecular Pathology, Yamaguchi University Graduate School of Medicine, Ube, Japan.
- KMID: 2348260
- DOI: http://doi.org/10.5946/ce.2015.131
Abstract
- A 64-year-old man was found to have a nodule in his right lung. He also complained of nausea and abdominal pain during the clinical course. Esophagogastroduodenoscopy revealed a duodenal ulcer associated with severe stenosis and a suspicion of malignancy. However, three subsequent biopsies revealed no evidence of malignancy. The fourth biopsy showed scattered large eosinophilic cells with an eccentric nucleus, leading to a diagnosis of Russell body duodenitis (RBD). RBD is an extremely rare disease, and little is known about its etiology and clinical course. The pathogenesis of RBD is discussed based on our experience with this case.
MeSH Terms
Figure
-

Fig. 1. (A) The first esophagogastroduodenoscopy revealed irregular ulceration in the duodenal bulb. The lumen was obstructed due to severe stenosis. (B) A biopsy was performed from the duodenal ulcer. Inflammatory cell infiltration, necrotic tissue, granulation tissue and large atypical cells were observed (H&E stain, ×200).

Fig. 2. Contrast-enhanced upper gastrointestinal radiography revealed severe stenosis from the duodenal bulb to the superior duodenal angulus.
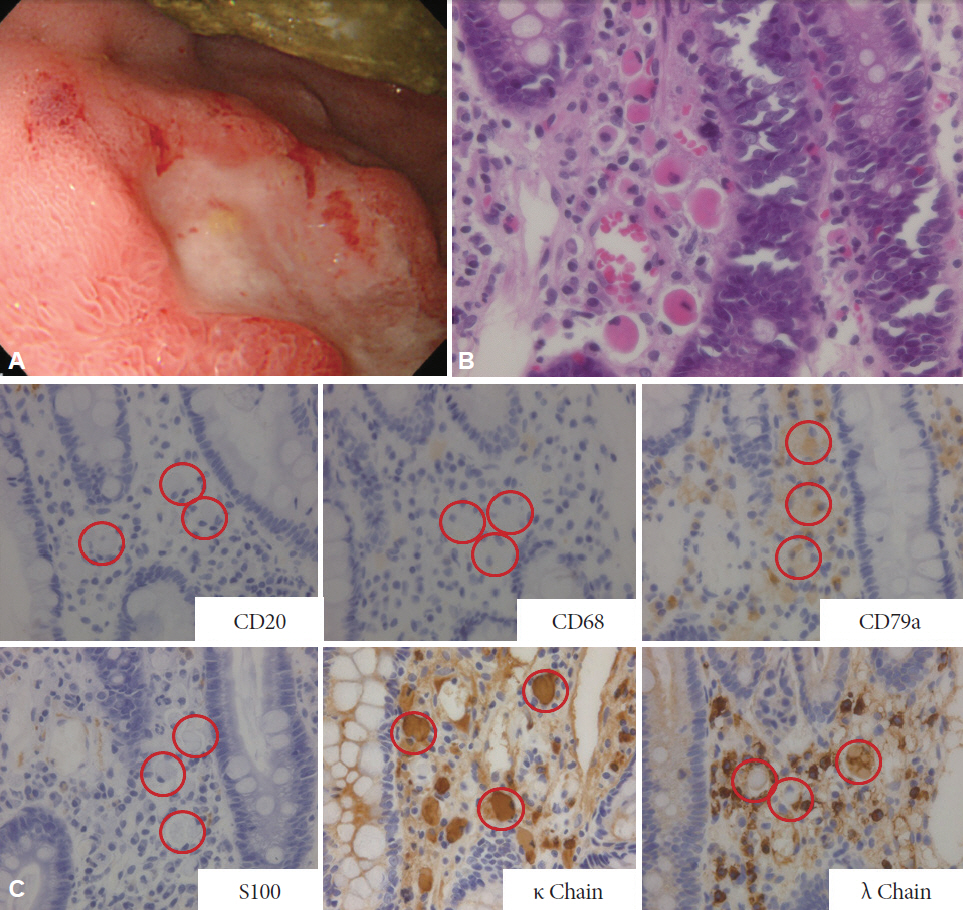
Fig. 3. (A) The fourth esophagogastroduodenoscopy. The peripheral redness and edema of ulcer became more severe than those in the previous findings. (B) The fourth biopsy from the duodenal ulcer revealed dissemination of large cells with eosinophilic cytoplasms and eccentric nuclei in the necrotic/granulation tissue of the duodenal lamina propria (H&E stain, ×200). (C) Immunostaining of the fourth biopsy (×200). The red circles indicate Russell body.

Fig. 4. (A) The fifth esophagogastroduodenoscopy. The ulcers in the duodenal bulb were reduced, some of which were scarred. (B) The fifth biopsy from the duodenal ulcer. Although the biopsy confirmed the presence of a few Russell bodies, the majority of those had disappeared (H&E stain, ×100).
Reference
-
1. Russell W. An address on a characteristic organism of cancer. Br Med J. 1890; 2:1356–1360.
Article2. Hsu SM, Hsu PL, McMillan PN, Fanger H. Russell bodies: a light and electron microscopic immunoperoxidase study. Am J Clin Pathol. 1982; 77:26–31.
Article3. Tazawa K, Tsutsumi Y. Localized accumulation of Russell body-containing plasma cells in gastric mucosa with Helicobacter pylori infection: ‘Russell body gastritis’. Pathol Int. 1998; 48:242–244.4. Savage NM, Fortson T, Schubert M, Chamberlain S, Lee J, Ramalingam P. Isolated Russell body duodenitis. Dig Dis Sci. 2011; 56:2202–2204.
Article5. Paniz Mondolfi A, Samuel M, Kikhney J, et al. Russell body duodenitis: a histopathological and molecular approach to a rare clinical entity. Pathol Res Pract. 2012; 208:415–419.
Article6. Takahashi Y, Shimizu S, Uraushihara K, Fukusato T. Russell body duodenitis in a patient with retroperitoneal metastasis of ureteral cancer. World J Gastroenterol. 2013; 19:125–128.
Article7. Zhang H, Jin Z, Cui R. Russell body gastritis/duodenitis: a case series and description of immunoglobulin light chain restriction. Clin Res Hepatol Gastroenterol. 2014; 38:e89–e97.
Article8. Munday WR, Kapur LH, Xu M, Zhang X. Russell body duodenitis with immunoglobulin kappa light chain restriction. World J Gastrointest Endosc. 2015; 7:73–76.
Article9. Bhaijee F, Brown KA, Long BW, Brown AS. Russell body gastroenteritis: an aberrant manifestation of chronic inflammation in gastrointestinal mucosa. Case Rep Med. 2013; 2013:797264.
Article10. Karabagli P, Gokturk HS. Russell body gastritis: case report and review of the literature. J Gastrointestin Liver Dis. 2012; 21:97–100.11. Del Gobbo A, Elli L, Braidotti P, Di Nuovo F, Bosari S, Romagnoli S. Helicobacter pylori-negative Russell body gastritis: case report. World J Gastroenterol. 2011; 17:1234–1236.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Russell Body Gastritis Treated by Helicobacter pylori Eradication
- Regression of Russell Body Gastritis after Helicobacter pylori Eradication
- Russell Body - Containing Plasma Cell Aggregations Mimiccking Signet Ring Cell Carcinoma of the Stomach
- Clinical and Pathologic Features of Nodular Duodenitis in Children
- Russell Body Gastritis Disappeared after Helicobacter pylori Eradication
