Various Imaging Features of Intestinal Malrotation, Associated Anomalies, and Complications
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Cheonan Hospital, Korea. ytokim@schca.ac.kr
Abstract
- An abnormal rotation or fixation of the small and large bowel may occur during development, and can result in various forms of intestinal malrotation. Intestinal malrotations are associated with anomalies such as heterotaxy and peritoneal encapsulation, as well as various other complications including midgut volvulus and an internal hernia. Gastrointestinal disorders occurring in patients with intestinal malrotation are difficult to diagnose because of the atypical symptoms and imaging features. We illustrate the various imaging features of intestinal malrotation, associated anomalies, and complications.
MeSH Terms
Figure
-
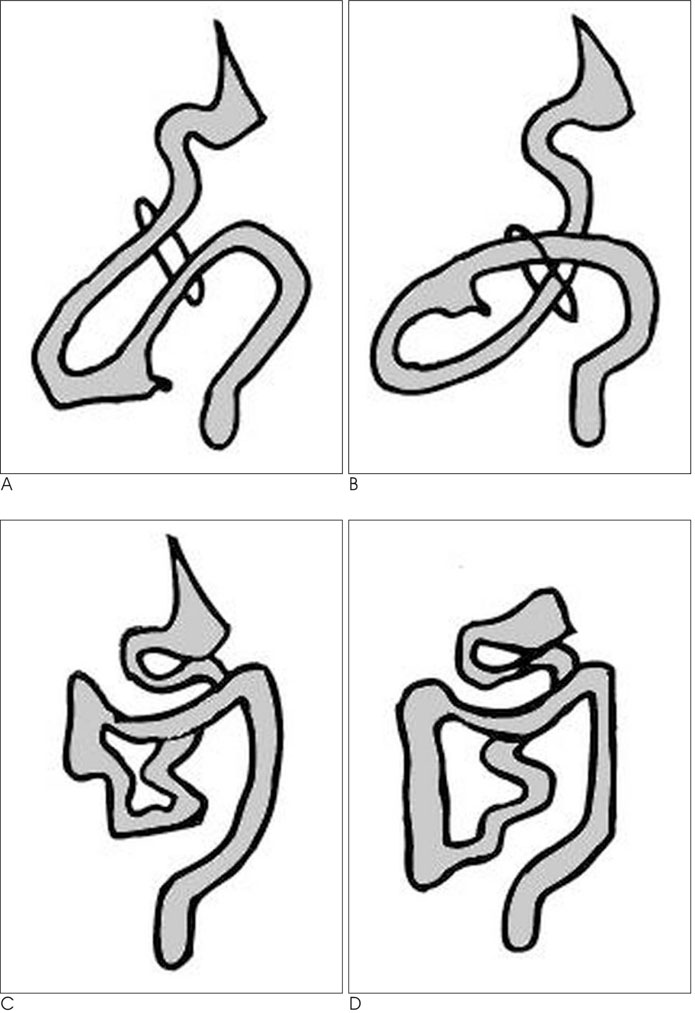
Fig. 1 Drawing of mid-gut rotation. A. Prior to 6 weeks the duodenum rotates 90° counterclockwise and lies to the right of the SMA. The cecum rotates 90° counterclockwise and lies to the left of the SMA. B. The duodenum rotates another 90° counterclockwise and lies posterior to the SMA. The rest of the midgut is in the umbilical cord. C. At 10 weeks, the intestines return to the peritoneal cavity. The final 90° counterclockwise rotation of the duodenum, with the duodeno-jejunal flexure lying to the right of the midline. The cecum rotates 180°. The right colon is the last portion of the gastrointestinal tract to rotate completely, allowing the cecum to descend into the right lower quadrant. D. The final stage is peritoneal fixation of bowel.
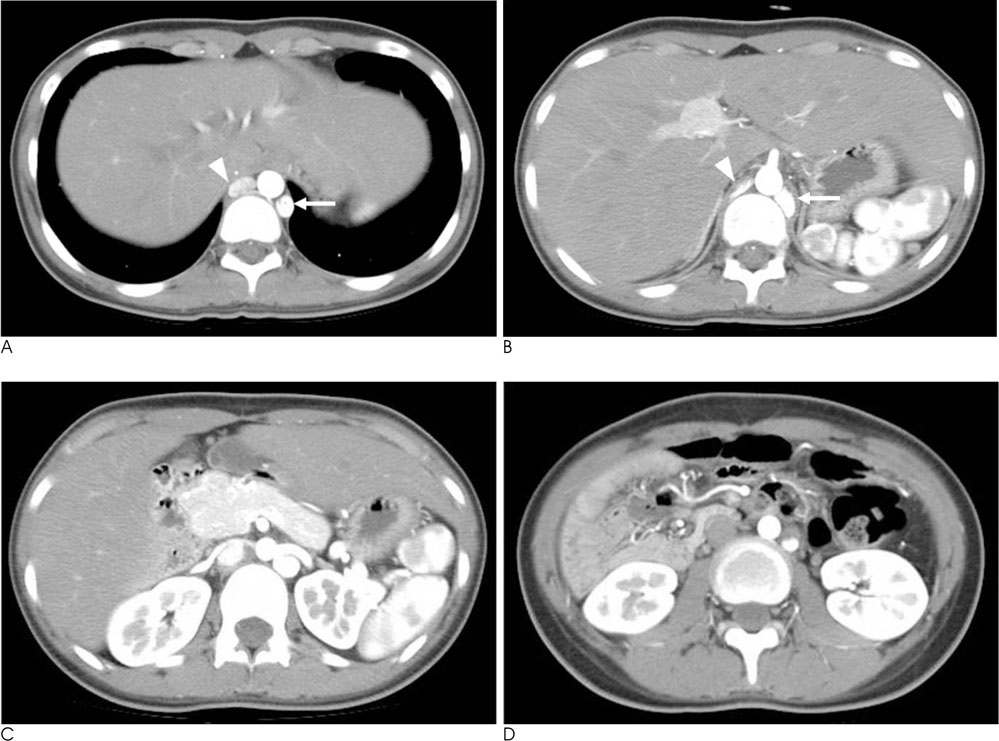
Fig. 2 Heterotaxy with intestinal malrotation in a 15-year-old girl. The patient presented with chronic, recurrent epigastric pain for three years. A, B. Axial CT scans show a non-visualized intrahepatic inferior vena cava, prominent hemiazygous (arrow) and azygous vein (arrowhead), and polysplenia. Azygous continuation with inferior vena cava interruption and polysplenia was diagnosed, associated with heterotaxy. C. Axial CT scan shows short pancreas and bilateral inferior vena cava. D. Axial CT scan shows the right sided small bowel and left sided colon. Abdominal pain improved after surgical removal of Ladd's band.
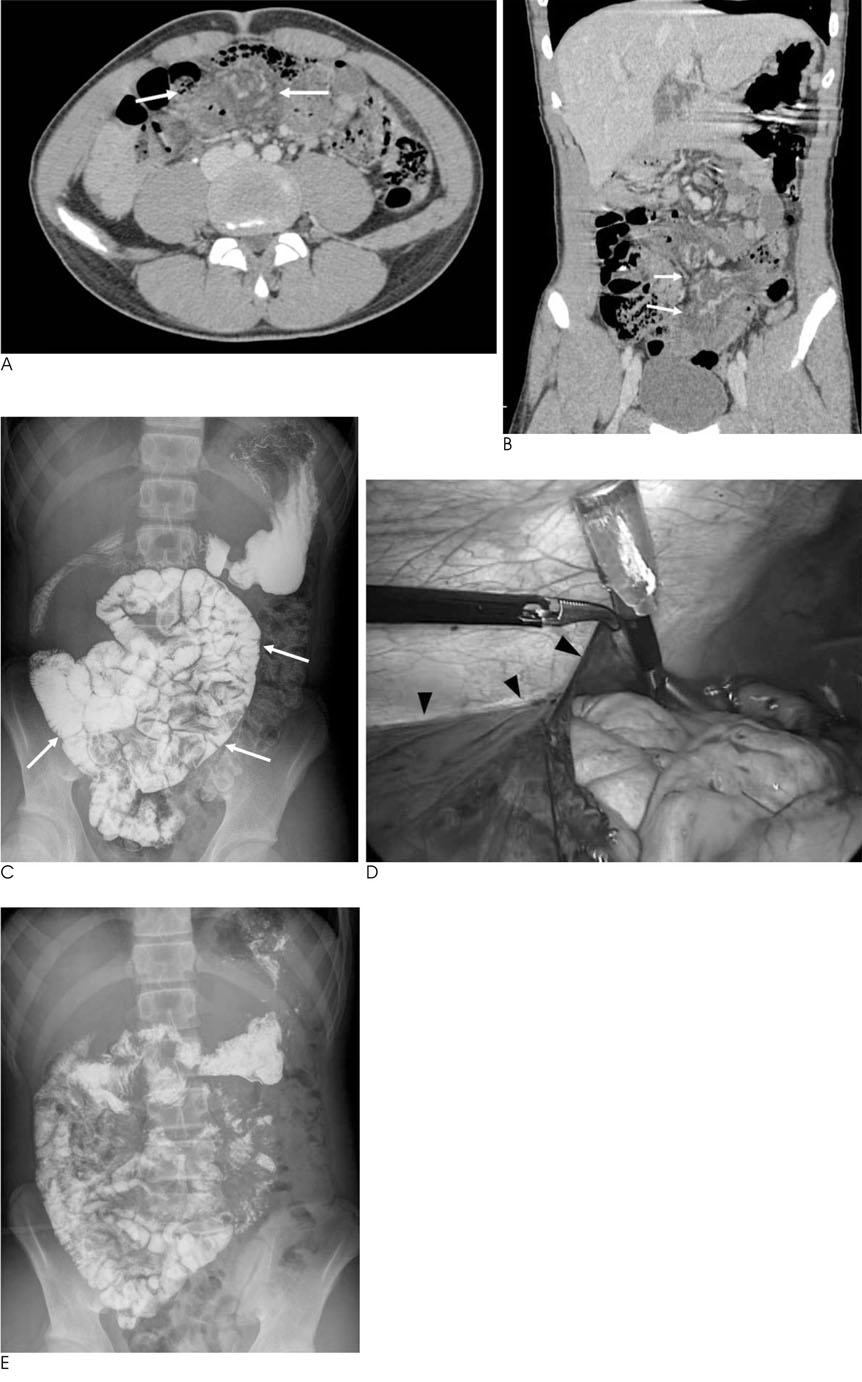
Fig. 3 Peritoneal encapsulation with intestinal malrotation in a 13-year-old boy. The patient presented with acute abdominal pain, nausea and vomiting for one day. A, B. Axial (A) and coronal multiplanar reformatted image (B) show congested mesenteric vessels and increased attenuation along the mesentery (arrows). C. Small bowel series shows an abdominal cocoon, and an aggregated and clustered small bowel (arrows). An abnormally located duodenojejunal junction is also seen. D. Intraoperative photograph shows nearly the entire small bowel encapsulated with a huge sac (arrowheads). E. Small bowel series after surgery shows that small bowel is not clustered.

Fig. 4 Malrotation with midgut volvulus in a 1-year-old girl. A. Precontrast CT scan after barium study shows a whirl-like appearance of the barium-filled small bowel loop (arrow) in the midline area of the mid abdomen. B, C. Postcontrast CT scans obtained seven days later show a whirlpool appearance of the superior mesenteric vein and small bowel around the superior mesenteric artery (B), and a barium-filled appendix in the midline of the mid abdomen (arrowhead) (C). D. Abdominal radiograph obtained on the same day as the CT shows a barium-filled appendix (arrowhead) in the right paramedian area of the mid abdomen.
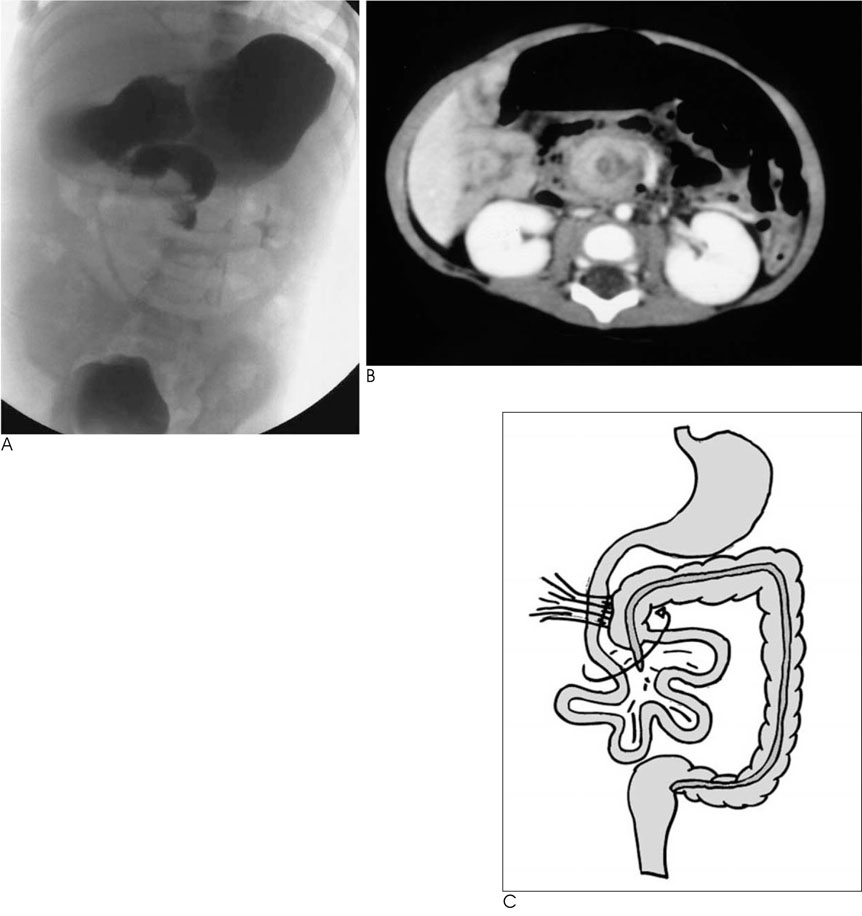
Fig. 5 Midgut volvulus with intestinal malrotation in a 1-year-old boy. A. Upper GI series shows a corkscrew appearance of the duodenum and upper jejunum. B. CT scan shows a whirlpool appearance of the superior mesenteric vein and small bowel around the superior mesenteric artery. C. Drawing shows that malrotation results in malposition of bowel and abnormal fibrous peritoneal bands of Ladd, which attach to right colon predispose to midgut volvulus. In this condition, the small intestine fails to return to the abdomen normally, and the mesenteries fail to undergo normal fixation. As a result, twisting of the intestines may occur.
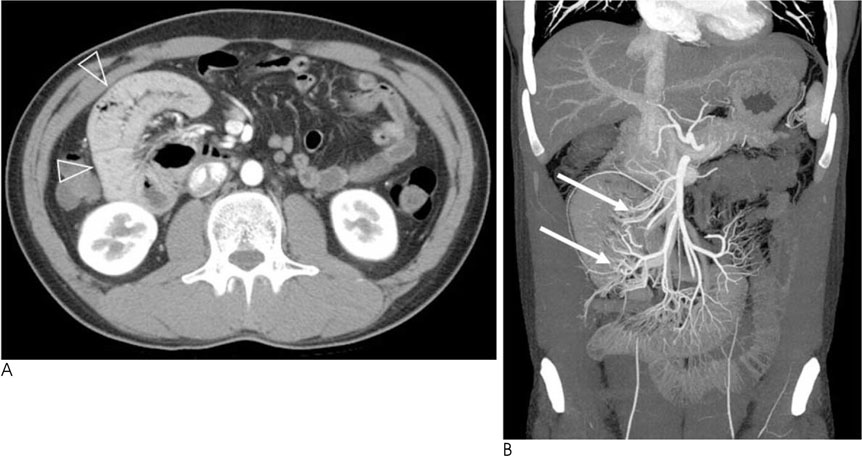
Fig. 6 Right paraduodenal hernia in a 30-year-old man. The patient presented with intermittent abdominal pain for 2 years. A. Axial CT scan shows bowel loops within sac like structure (arrowheads) in right abdominal cavity. B. Coronal multiplanar reformatted image shows abnormally located jejunal branches (arrows) of superior mesenteric artery. Normally jejunal branches course to left upper abdomen.
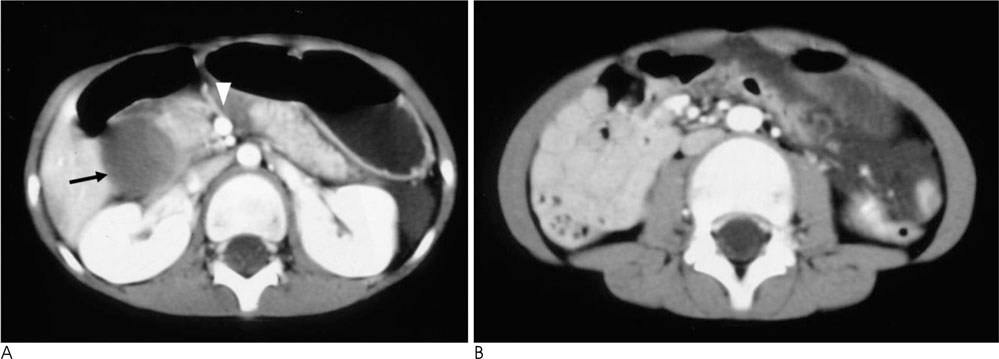
Fig. 7 Duodenal hematoma caused by traffic accident in a 7-year-old boy. The patient was diagnosed incidentally with nonrotation of the bowel on a CT scan. A. CT scan shows a hematoma (arrow) of the duodenal second loop, and a vertically oriented SMA-SMV relationship (arrowhead). B. CT scan at the level of mid-abdomen shows the small bowel on the right side.

Fig. 8 Periappendiceal abscess with intestinal malrotation in a 37-year-old man. A. Axial CT scan shows irregular low density lesion with fat infiltration (arrowhead) in pelvic cavity. B. Coronal multiplanar reformatted image shows right sided small bowel and left sided large bowel. Base of appendix (arrow) is seen adjacent the low density lesion with fat infiltration (arrowhead).

Fig. 9 Appendicitis in a 7-year-old boy with intestinal malrotation. A. CT scan shows fluid filled appendix (arrow) with surrounding peri-appendiceal inflammation in the mid-abdomen. B. CT scan shows the small bowel in right abdomen and large bowel in left abdomen. C. Upper gastrointestinal series shows the jejunal loops in the right abdomen. Note that the duodenum does not cross the midline. D. 2 hour delayed film shows abnormally located ileocecal junction (arrowhead) in left lower abdomen. Note small bowel in right abdomen and large bowel in left abdomen.
Reference
-
1. Applegate KE, Anderson JM, Klatte EC. Intestinal malrotation in children: a problem-solving approach to the upper gastrointestinal series. Radiographics. 2006; 26:1485–1500.2. Gore RM, Levine MS. Textbook of gastrointestinal radiology. 3rd ed. Philadelphia: Saunders;2008. p. 2188–2192.3. Pickhardt PJ, Bhalla S. Intestinal malrotation in adolescents and adults: spectrum of clinical and imaging features. AJR Am J Roentgenol. 2002; 179:1429–1435.4. Slovis TL. Caffey's pediatric diagnostic imaging. 11th ed. Philadelphia: Mosby/Elsevier;2008. p. 2106–2116.5. Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics. 2002; 22:1439–1456.6. Chew MH, Sophian Hadi I, Chan G, Ong HS, Wong WK. A problem encapsulated: the rare peritoneal encapsulation syndrome. Singapore Med J. 2006; 47:808–810.7. Wig JD, Gupta SK. Computed tomography in abdominal cocoon. J Clin Gastroenterol. 1998; 26:156–157.8. Tombak MC, Apaydin FD, Colak T, Duce MN, Balci Y, Yazici M, et al. An unusual cause of intestinal obstruction: abdominal cocoon. AJR Am J Roentgenol. 2010; 194:W176–W178.9. Lin JN, Lou CC, Wang KL. Intestinal malrotation and midgut volvulus: a 15-year review. J Formos Med Assoc. 1995; 94:178–181.10. Welte FJ, Grosso M. Left-sided appendicitis in a patient with congenital gastrointestinal malrotation: a case report. J Med Case Rep. 2007; 1:92.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Sided Appendicitis in Patient with Intestinal Malrotation
- A Case of Duodenal Web Associated with Intestinal Malrotation
- Malrotation and Midgut Volvulus in Children: Diagnostic Approach, Imaging Findings, and Pitfalls
- Midgut Volvulus in a 70-year-old Man Due to Intestinal Nonrotation
- Malrotation complicating Midgut Volvulus: Ultrasonographic Finding
