A Rathke's Cleft Cyst with Chronic Inflammation Mimicking a Pituitary Macroadenoma
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. ahn-kj@catholic.ac.kr
- 2Department of Neurosurgery, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea.
Abstract
- Rathke's cleft cyst is a benign cystic lesion arising in the sellar or suprasellar region. Most cases of Rathke's cleft cysts are thin-walled cystic lesions, but in rare cases, can cause a pituitary abscess by inflammation or infection. We report on a case of Rathke's cleft cyst with chronic inflammation mimicking a pituitary macroadenoma seen as a thick-walled irregular cystic lesion on brain CT and MRI.
Figure
-
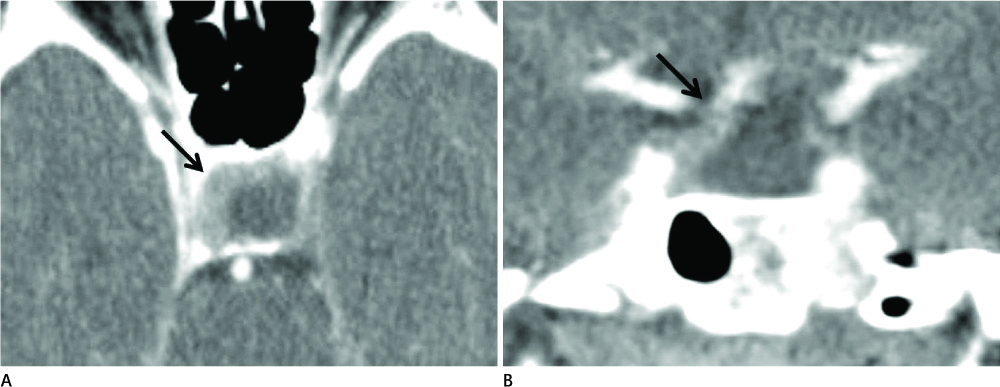
Fig. 1 CT on admission. A, B. Contrast enhanced CT images show well defined cystic mass (arrow) in the sellar and suprasellar areas with asymmetric thick rim enhancement.
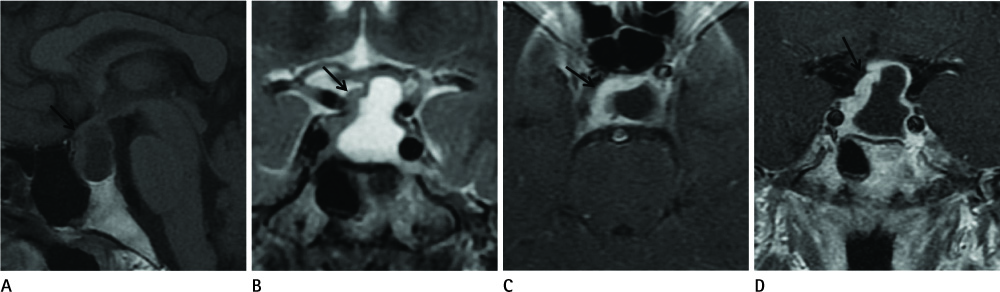
Fig. 2 MRI on admission. A. T1-weighted sagittal image shows cystic mass (arrow) in the sellar and suprasellar area. Normal or compressed pituitary gland is not detected. B. T2-weighted coronal image shows intermediate signal intensity mass (arrow) with internal cystic component, similar signal to the CSF. D. Contrast enhanced T1-weighted axial and coronal images show thick rim enhancement of the peripheral solid portion of the mass (arrow). Note.-CSF = cerebrospinal fluid
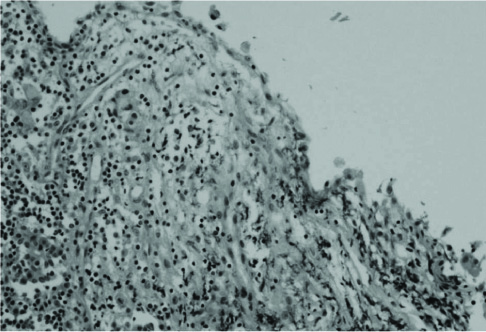
Fig. 3 Microscopic finding shows lining epithelium consisting of cuboidal or flat cells with subepithelial inflammatory cell infiltration including lymphocytes and histiocytes.
Reference
-
1. Bognàr L, Szeifert GT, Fedorcsàk I, Pàsztor E. Abscess formation in Rathke's cleft cyst. Acta Neurochir (Wien). 1992; 117:70–72.2. Sato M, Matsushima Y, Taguchi J, Matsumoto S, Tatsumi C, Ozaki M, et al. [A case of pituitary abscess caused by infection of Rathke's cleft cyst]. No Shinkei Geka. 1995; 23:991–995.3. Brassier G, Morandi X, Tayiar E, Riffaud L, Chabert E, Heresbach N, et al. Rathke's cleft cysts: surgical-MRI correlation in 16 symptomatic cases. J Neuroradiol. 1999; 26:162–171.4. Rhee JJ, Kim JH, Kim CJ, Lee JK, Jung HW. Radiological characteristics in Rathke's cleft cyst. J Korean Neurosurg Soc. 2003; 34:140–145.5. Naylor MF, Scheithauer BW, Forbes GS, Tomlinson FH, Young WF. Rathke cleft cyst: CT, MR, and pathology of 23 cases. J Comput Assist Tomogr. 1995; 19:853–859.6. Voelker JL, Campbell RL, Muller J. Clinical, radiographic, and pathological features of symptomatic Rathke's cleft cysts. J Neurosurg. 1991; 74:535–544.7. Ciappetta P, Calace A, D'Urso PI, De Candia N. Endoscopic treatment of pituitary abscess: two case reports and literature review. Neurosurg Rev. 2008; 31:237–246. discussion 246.8. Domingue JN, Wilson CB. Pituitary abscesses. Report of seven cases and review of the literature. J Neurosurg. 1977; 46:601–608.9. Jain KC, Varma A, Mahapatra AK. Pituitary abscess: a series of six cases. Br J Neurosurg. 1997; 11:139–143.10. Takao H, Doi I, Watanabe T. Diffusion-weighted magnetic resonance imaging in pituitary abscess. J Comput Assist Tomogr. 2006; 30:514–516.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pituitary Tumors Composed of Adenohypophysial Adenoma and Rathke's Cleft Cyst Elements
- A Rathke's Cleft Cyst Presenting with Apoplexy
- Symptomatic Rathke's Cleft Cyst in the Interpeduncular Cistern: Case Report
- The Endocrinological Characteristics of Rathke's Cleft Cyst: Pathologically Confirmed in Seven Cases
- A Case of Rathke Cleft Cyst Apoplexy
