A Rathke's Cleft Cyst Presenting with Apoplexy
- Affiliations
-
- 1Department of Neurosurgery, Keimyung University School of Medicine, Dongsan Medical Center, Daegu, Korea. bach1158@dsmc.or.kr
- KMID: 2190660
- DOI: http://doi.org/10.3340/jkns.2012.52.4.404
Abstract
- The occurrence of symptomatic pituitary hemorrhage into a Rathke's cleft cyst (RCC) is extremely rare. The author reports an interesting case of intra- and suprasellar RCC presented with features of pituitary apoplexy. This 62-year-old woman suffered acute headache, mental confusion, and partial hypopituitarism. The characteristics of the magnetic resonance imaging seemed most compatible with a hemorrhagic pituitary adenoma. Transsphenoidal drainage of the cyst contents confirmed the diagnosis of hemorrhagic RCC and resolved the symptoms. All published data on this rare clinical entity are extracted and reviewed.
Keyword
MeSH Terms
Figure
-
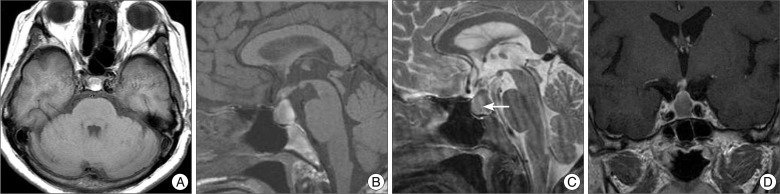
Fig. 1 Preoperative magnetic resonance images of a patient presented with pituitary apoplexy. The lesion is mainly isointense with some hyperintense foci on T1-weighted images (A and B). A fluid level (arrow) with isointense signal anteriorly and hypointense signal posteriorly is noted on sagittal T2-weighted image (C). It displays rim enhancement surrounding the cyst following gadolinium infusion (D).
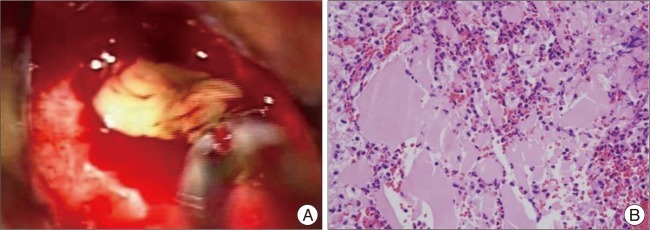
Fig. 2 A : Operative and pathology features of a hemorrhagic Rathke's cleft cyst. At surgery, an initial gush of hemorrhagic fluid was followed by a thick yellowish mucinous substance. B : Histopatholgical examination demonstrates a benign cyst consisting of columnar and cuboidal epitheliums and amorphous cyst contents with acute hemorrhages.
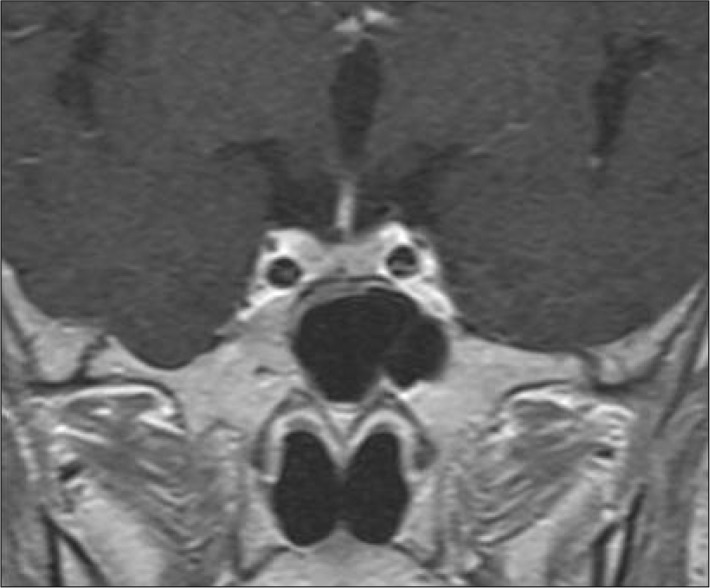
Fig. 3 Follow-up magnetic resonance images taken 6 years after surgery show no evidence of cyst recurrence.
Reference
-
1. Aho CJ, Liu C, Zelman V, Couldwell WT, Weiss MH. Surgical outcomes in 118 patients with Rathke cleft cysts. J Neurosurg. 2005; 102:189–193. PMID: 15739543.
Article2. Albini CH, MacGillivray MH, Fisher JE, Voorhess ML, Klein DM. Triad of hypopituitarism, granulomatous hypophysitis, and ruptured Rathke's cleft cyst. Neurosurgery. 1988; 22(1 Pt 1):133–136. PMID: 3344071.
Article3. Benveniste RJ, King WA, Walsh J, Lee JS, Naidich TP, Post KD. Surgery for Rathke cleft cysts : technical considerations and outcomes. J Neurosurg. 2004; 101:577–584. PMID: 15481709.4. Billeci D, Marton E, Tripodi M, Orvieto E, Longatti P. Symptomatic Rathke's cleft cysts : a radiological, surgical and pathological review. Pituitary. 2004; 7:131–137. PMID: 16328563.
Article5. Binning MJ, Gottfried ON, Osborn AG, Couldwell WT. Rathke cleft cyst intracystic nodule : a characteristic magnetic resonance imaging finding. J Neurosurg. 2005; 103:837–840. PMID: 16304987.
Article6. Binning MJ, Liu JK, Gannon J, Osborn AG, Couldwell WT. Hemorrhagic and nonhemorrhagic Rathke cleft cysts mimicking pituitary apoplexy. J Neurosurg. 2008; 108:3–8. PMID: 18173304.
Article7. Chaiban JT, Abdelmannan D, Cohen M, Selman WR, Arafah BM. Rathke cleft cyst apoplexy : a newly characterized distinct clinical entity. J Neurosurg. 2011; 114:318–324. PMID: 20509729.
Article8. Komatsu F, Tsugu H, Komatsu M, Sakamoto S, Oshiro S, Fukushima T, et al. Clinicopathological characteristics in patients presenting with acute onset of symptoms caused by Rathke's cleft cysts. Acta Neurochir (Wien). 2010; 152:1673–1678. PMID: 20495985.
Article9. Kurisaka M, Fukui N, Sakamoto T, Mori K, Okada T, Sogabe K. A case of Rathke's cleft cyst with apoplexy. Childs Nerv Syst. 1998; 14:343–347. PMID: 9726587.
Article10. Lee HJ, Kalnin AJ, Holodny AI, Schulder M, Grigorian A, Sharer LR. Hemorrhagic chondroid chordoma mimicking pituitary apoplexy. Neuroradiology. 1998; 40:720–723. PMID: 9860121.
Article11. Nishioka H, Haraoka J, Izawa H, Ikeda Y. Headaches associated with Rathke's cleft cyst. Headache. 2006; 46:1580–1586. PMID: 17115992.
Article12. Nishioka H, Ito H, Miki T, Hashimoto T, Nojima H, Matsumura H. Rathke's cleft cyst with pituitary apoplexy : case report. Neuroradiology. 1999; 41:832–834. PMID: 10602857.
Article13. Oka H, Kawano N, Suwa T, Yada K, Kan S, Kameya T. Radiological study of symptomatic Rathke's cleft cysts. Neurosurgery. 1994; 35:632–636. discussion 636-637. PMID: 7808605.
Article14. Onesti ST, Wisniewski T, Post KD. Pituitary hemorrhage into a Rathke's cleft cyst. Neurosurgery. 1990; 27:644–646. PMID: 2234374.
Article15. Pawar SJ, Sharma RR, Lad SD, Dev E, Devadas RV. Rathke's cleft cyst presenting as pituitary apoplexy. J Clin Neurosci. 2002; 9:76–79. PMID: 11749024.
Article16. Rosales MY, Smith TW, Safran M. Hemorrhagic Rathke's cleft cyst presenting as diplopia. Endocr Pract. 2004; 10:129–134. PMID: 15256330.
Article
