Korean Circ J.
2016 Jul;46(4):522-529. 10.4070/kcj.2016.46.4.522.
The Relationship between P & QT Dispersions and Presence & Severity of Stable Coronary Artery Disease
- Affiliations
-
- 1Department of Cardiology, Erzurum Region Training and Research Hospital, Erzurum, Turkey. bng_dlkc@hotmail.com
- 2Department of Internal Medicine, CerrahpaÅŸa Faculty of Medicine, Istanbul University, Istanbul, Turkey.
- 3Department of Cardiology, Istanbul Siyami Ersek Training and Research Hospital, Istanbul, Turkey.
- 4Department of Cardiology, Istanbul Bilim University, Istanbul, Turkey.
- KMID: 2344427
- DOI: http://doi.org/10.4070/kcj.2016.46.4.522
Abstract
- BACKGROUND AND OBJECTIVES
The study aimed to evaluate the correlation between electrocardiographic (ECG) parameters and presence and extent of coronary artery disease (CAD) to indicate the usefulness of these parameters as predictors of severity in patients with stable CAD.
SUBJECTS AND METHODS
Two hundred fifty patients, without a history of any cardiovascular event were included in the study. The ECG parameters were measured manually by a cardiologist before coronary angiography. The patients were allocated into five groups: those with normal coronary arteries (Group 1), non-critical coronary lesions (Group 2), one, two and three vessel disease (Group 3, Group 4 and Group 5, respectively.
RESULTS
Group 1 had the lowest P wave dispersion (PWD) and P wave (Pmax), QT interval (QTmax), QT dispersion (QTd), corrected QT dispersion (QTcd) and QT dispersion ratio (QTdR), while the patients in group 5 had the highest values of these parameters. Gensini score and QTmax, QTd, QTcmax, QTcd, QTdR, Pmax, and PWD were positively correlated. QTdR was the best ECG parameter to differentiate group 1 and 2 from groups with significant stenosis (groups 3, 4, and 5) (area under curve [AUC] 0.846). QTdR was the best ECG parameter to detect coronary arterial narrowing lesser than 50% and greater than 50%, respectively (AUC 0.858).
CONCLUSION
Presence and severity of CAD can be determined by using ECG in patients with stable CAD and normal left ventricular function.
MeSH Terms
Figure
-
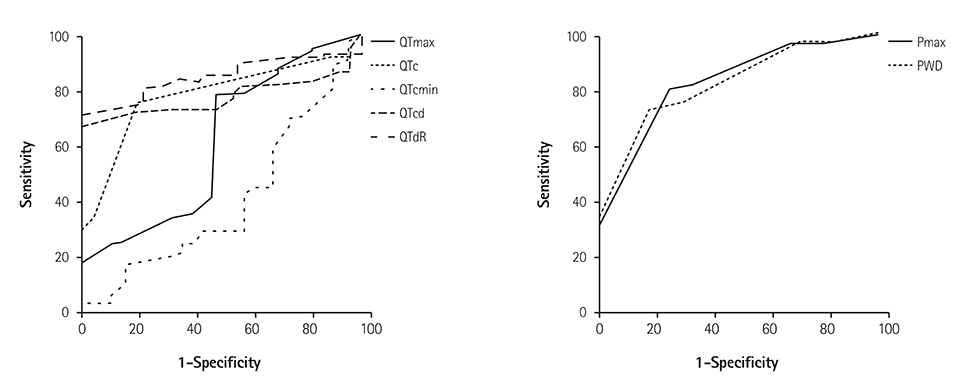
Fig. 1 ROC Curve of electrocardiographic parameters that distinguished normal coronary from non-critical and significant stenosis groups. QTmax: maximum QT interval, QTd: QT dispersion, QTcmax: corrected QT maximum interval, QTcd: corrected QT dispersion, QTdR: QT dispersion ratio, Pmax: maximum p wave interval, PWD: P wave dispersion.
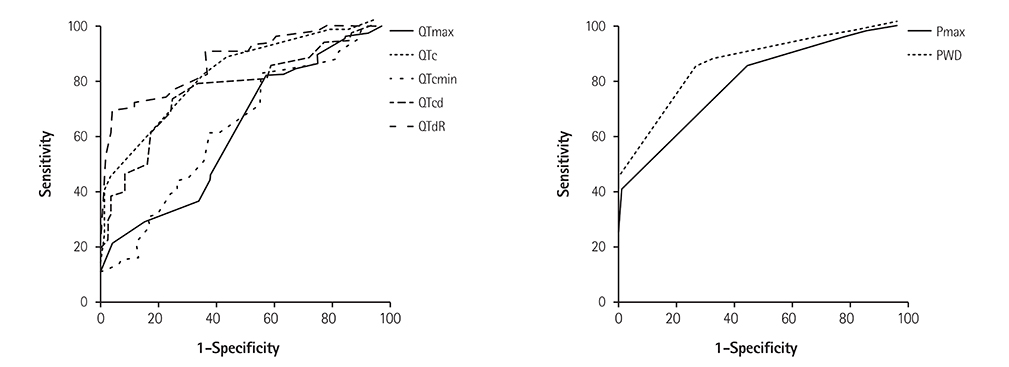
Fig. 2 ROC Curve of electrocardiographic parameters that distinguished coronary arteries with <50% narrowing from the ones with ≥50% narrowing. QTc: corrected QT, QTmax: maximum QT interval, QTcmax: corrected QT maximum interval, QTcd: corrected QT dispersion, QTdR: QT dispersion ratio, Pmax: maximum p wave interval, PWD: P wave dispersion.
Reference
-
1. Napoli C, Glass CK, Witztum JL, Deutsch R, D'Armiento FP, Palinski W. Influence of maternal hypercholesterolemia during pregnancy on progression of early atherosclerotic lesions in childhood: Fate of Early Lesions in Children (FELIC) study. Lancet. 1999; 354:1234–1241.2. Task Force Members. Montalescot G, Sechtem U, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013; 34:2949–3003.3. Dilaveris PE, Gialafos EJ, Sideris SK, et al. Simple electrocardiographic markers for the prediction of paroxysmal idiopathic atrial fibrillation. Am Heart J. 1998; 135(5 Pt 1):733–738.4. Day CP, McComb LM, Campbell RW. QT dispersion: an indication of arrhythmia risk in patients with long QT intervals. Br Heart J. 1990; 63:342–344.5. Savelieva I, Camm AJ, Malik M. Gender-specific differences on QT dispersion measured in 1100 healthy subjects. (abstr). PACE. 1999; 22:885.6. Higham PD, Furniss SS, Campbell RW. QT dispersion and components of the QT interval in ischemia and infarction. Br Heart J. 1995; 73:32–36.7. Glancy JM, Garrat CJ, de Bono DP. Dynamics of QT dispersion during myocardial infarction and ischemia. Int J Cardiol. 1996; 57:55–60.8. Sporton SC, Taggart P, Sutton PM, Walker JM, Hardman SM. Acute ischemia: a dynamic influence on QT dispersion. Lancet. 1997; 349:306–309.9. Beaubien ER, Pylypchuk GB, Akhtar J, Biem HJ. Value of corrected QT interval dispersion in identifying patients initiating dialysis at increased risk of total and cardiovascular mortality. Am J Kidney Dis. 2002; 39:834–842.10. Naas AA, Davidson NC, Thompson C, et al. QT and QTc dispersion are accurate predictors of cardiac death in newly diagnosed non-insulin-dependent diabetes: cohort study. BMJ. 1998; 316:745–746.11. Malik M, Batchvarov VN. Measurement, interpretation, and clinical potential of QT dispersion. J Am Coll Cardiol. 2000; 36:1749–1766.12. Emond M, Mock MB, Davis KB, et al. Long-term survival of medically treated patients in the Coronary Artery Surgery Study (CASS) registry. Circulation. 1994; 90:2645–2657.13. Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983; 51:606.14. Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A. Myocardial infarction and coronary deaths in the World Health Organization MONICA Project. Registration procedures, event rates, and case-fatality rates in 38 populations from 21 countries in four continents. Circulation. 1994; 90:583–612.15. Kannel WB, Doyle JT, McNamara PM, Quickenton P, Gordon T. Precursors of sudden coronary death. Factors related to the incidence of sudden death. Circulation. 1975; 51:606–613.16. Risk stratification and survival after myocardial infarction. N Engl J Med. 1983; 309:331–336.17. Sanz G, Castañer A, Betriv A, et al. Determinants of prognosis in survivors of myocardial infarction: a prospective clinical angiographic study. N Engl J Med. 1982; 306:1065–1070.18. Hull SS Jr, Evans AR, Vanoli E, et al. Heart rate variability before and after myocardial infarction in conscious dogs at high and low risk of sudden death. J Am Coll Cardiol. 1990; 16:978–985.19. Kautzner J, Malik M. QT interval dispersion and its clinical utility. Pacing Clin Electrophysiol. 1997; 20:2625–2640.20. Day CP, McComb JM, Campell RW. QT dispersion: an indication of arrhytmia risk in patients with long QT intervals. Br Heart J. 1990; 63:342–344.21. Day CP, McComb JM, Campell RW. QT dispersion in sinus beats and ventricular extrasystoles in normal hearts. Br Heart J. 1992; 67:39–41.22. Elming H, Holm E, Jun L, et al. The prognostic value of the QT interval and QT interval dispersion in all-cause and cardiac mortality and morbidity in a population of Danish citizens. Eur Heart J. 1998; 19:1391–1400.23. Akyuz A, Alpsoy S, Akkoyun DC, Degirmenci H, Guler N. Maximal exercise-corrected QT as a predictor of coronary artery disease: comparison of simpler heart rate corrections. Korean Circ J. 2013; 43:655–663.24. Elsässer A, Schlepper M, Klövekorn WP, et al. Hibernating myocardium: an incomplete adaptation to ischemia. Circulation. 1997; 96:2920–2931.25. Zareba W, Moss AJ, le Cessie S. Dispersion of ventricular repolarization and arrhythmic death in coronary artery disease. Am J Cardiol. 1994; 74:550–553.26. Batur MK, Aksöyek S, Oto A, et al. Circadian variations of QTc dispersion: is it a clue to morning increase of sudden cardiac death? Clin Cardiol. 1999; 22:103–106.27. Lowe MD, Rowland E, Grace AA. QT dispersion and triple vessel coronary disease. Lancet. 1997; 349:1175–1176.28. Sporton SC, Taggart P, Sutton PM, Walker JM, Hardman SM. Acute ischemia: a dynamic influence on QT dispersion. Lancet. 1997; 349:306–309.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Relationship of the LV Systolic Function, the LV Dimension and the LV Mass to QT Dispersion in Stable Angina Patients who are with or without Significant Coronary Stenosis
- Association of a Corrected QT Interval with the Carotid Intima-Media Thickness and the Severity of Coronary Artery Disease in Patients with Coronary Artery Disease
- Maximal Exercise-Corrected QT as a Predictor of Coronary Artery Disease: Comparison of Simpler Heart Rate Corrections
- Difference of Systemic Vascular Compliance According to the Severity of Coronary Artery Disease in Ischemic Heart Disease
- Pain and Associated Symptoms in Patients with Acute Coronary Syndrome and Stable Coronary Artery Diseases: A Comparative Study
