Maximal Exercise-Corrected QT as a Predictor of Coronary Artery Disease: Comparison of Simpler Heart Rate Corrections
- Affiliations
-
- 1Department of Cardiology, Namik Kemal University Medical School, Tekirdag, Turkey. ayakyuzq5@gmail.com
- KMID: 1826556
- DOI: http://doi.org/10.4070/kcj.2013.43.10.655
Abstract
- BACKGROUND AND OBJECTIVES
The relationship between QT prolongation and myocardial ischemia is widely known. Due to the limited value of ST depression, we aimed to evaluate, by using four simpler heart rate corrections (Bazett, Framingham, Fridericia and Hodges), the value of maximal exercise-QTc prolongation in the diagnosis of coronary artery disease (CAD) presence and severity.
SUBJECTS AND METHODS
We enrolled 234 subjects (mean age 57.3+/-9 years, 143 men) who had undergone exercise testing and coronary angiography due to a suspicion of CAD in the study. Evaluating CAD severity with Gensini scoring, the CAD group (n=122) and controls with non-CAD were compared in terms of corrected QT duration at maximal exercise.
RESULTS
Age, gender, hypertension, dyslipidemia, smoking, exercise duration, resting, and peak heart rate were similar between the two groups (all p>0.05). The CAD group had higher raw QT values than the controls {268 (169-438) vs. 240 (168-348), p<0.001}. Although Framingham QTc of > or =350 ms and Fridericia QTc of > or =340 ms were seen to be useful for the diagnosis of CAD, there was no additive diagnostic value of exercise QTc in addition to ST depression. Maximal exercise-QTc Bazett (r=0.163, p=0.01), Framingham (r=0.239, p=0.001), and Fridericia (r=0.206, p=0.001) equations were weakly positively correlated with Gensini scoring.
CONCLUSION
The patients with CAD have longer QTc intervals at peak heart rates during exercise. This finding provides insufficient evidence to support routine incorporation of QTc at peak heart rates into exercise test interpretation.
Keyword
MeSH Terms
Figure
-
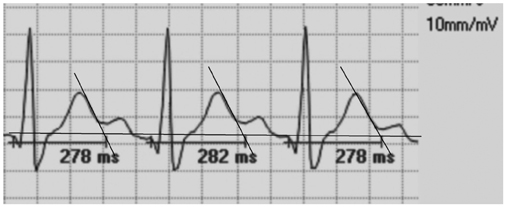
Fig. 1 Illustrates the representative example of exercise raw QT measurement at 50 mm/s paper speed.
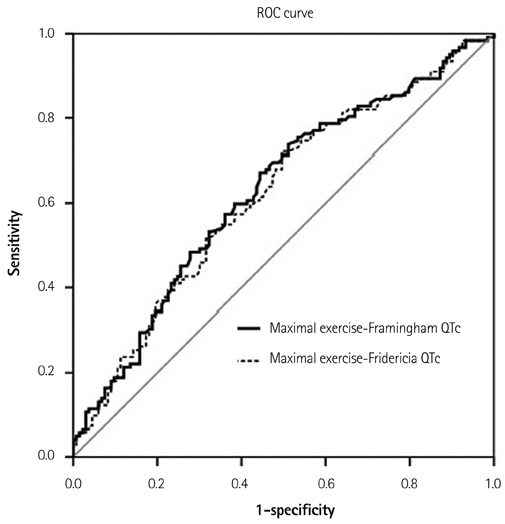
Fig. 2 The sensitivity and specificity of the Framingham and Fridericia formulae in the ROC curve. For the Framingham of ≥350 ms, the area under the curve (AUC): 0.628±0.035 (0.559-0.696), p<0.01 and for the Fridericia QTc: AUC: 0.620±0.035 (0.551-0.688), p<0.01. ROC: receiver operating characteristic.
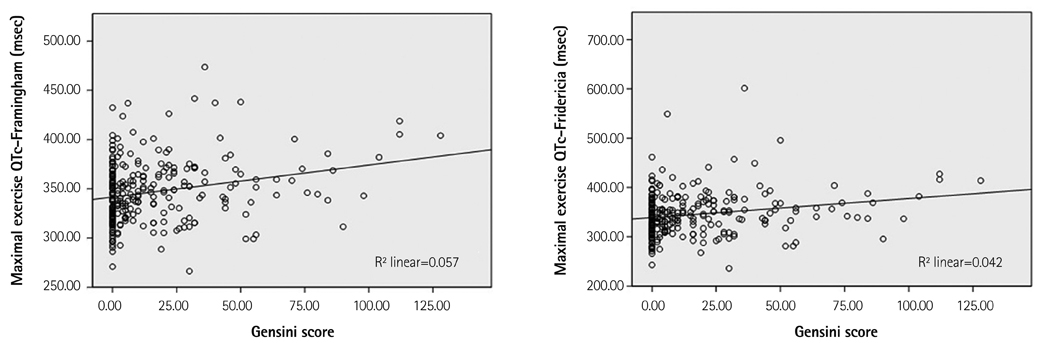
Fig. 3 Shows a positive linear relationship between Gensini scoring and maximal exercise QTc according to the Framingham (r=0.239, p=0.001) and Fridericia formulae (r=0.206, p=0.001).
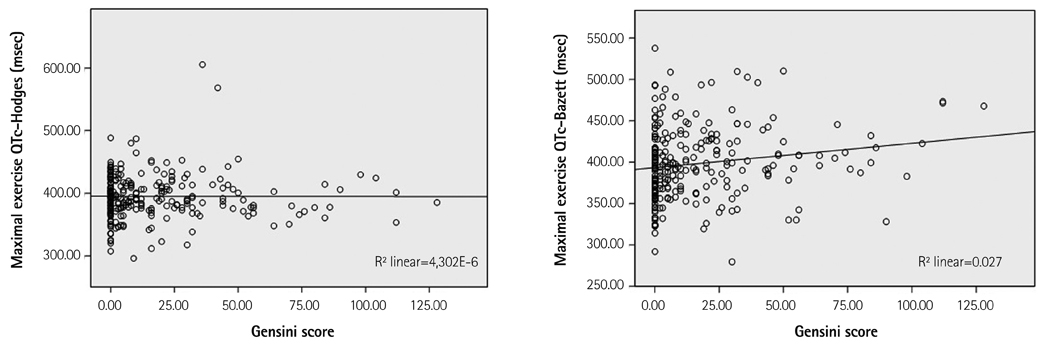
Fig. 4 Gensini scoring is not correlated with maximal exercise QTc according to the Hodges formula (r=0.001, p=0.989), but there is a weakly positive linear relationship between Gensini scoring and maximal exercise QTc according to Bazett (r=0.163, p=0.01).
Reference
-
1. Crow RS, Hannan PJ, Folsom AR. Prognostic significance of corrected QT and corrected JT interval for incident coronary heart disease in a general population sample stratified by presence or absence of wide QRS complex: the ARIC Study with 13 years of follow-up. Circulation. 2003; 108:1985–1989.2. Rickards AF, Norman J. Relation between QT interval and heart rate. New design of physiologically adaptive cardiac pacemaker. Br Heart J. 1981; 45:56–61.3. Davey P, Bateman J. Heart rate and catecholamine contribution to QT interval shortening on exercise. Clin Cardiol. 1999; 22:513–518.4. Schijvenaars BJ, van Herpen G, Kors JA. Intraindividual variability in electrocardiograms. J Electrocardiol. 2008; 41:190–196.5. Sohaib SM, Papacosta O, Morris RW, Macfarlane PW, Whincup PH. Length of the QT interval: determinants and prognostic implications in a population-based prospective study of older men. J Electrocardiol. 2008; 41:704–710.6. Bazett HC. An analysis of the time-relations of electrocardiograms. Heart. 1920; 7:353–370.7. Fridericia LS. Die systolendauer im elektrokardiogramm bei normalen menschen und bei herzkranken. Acta Med Scan. 1920; 53:469–486.8. Hodges M, Salerno D, Erlinen D. Bazett's QT correction reviewed-Evidence that a linear QT correctionfor heart is better. J Am Coll Cardiol. 1983; 12:694.9. Sagie A, Larson MG, Goldberg RJ, Bengtson JR, Levy D. An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol. 1992; 70:797–801.10. Rautaharju PM, Surawicz B, Gettes LS, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009; 53:982–991.11. Miranda CP, Liu J, Kadar A, et al. Usefulness of exercise-induced ST-segment depression in the inferior leads during exercise testing as a marker for coronary artery disease. Am J Cardiol. 1992; 69:303–307.12. Takase B, Masaki N, Hattori H, Ishihara M, Kurita A. Usefulness of automatic QT dispersion measurement for detecting exercise-induced myocardial ischemia. Anadolu Kardiyol Derg. 2009; 9:189–195.13. Ulgen MS, Karadede A, Alan S, Temamogğulari AV, Karabulut A, Toprak N. Contribution of the peak exercise QT dispersion to the accuracy of an exercise test during the evaluation of coronary artery disease. Acta Cardiol. 2000; 55:335–339.14. Chugh SS, Reinier K, Singh T, et al. Determinants of prolonged QT interval and their contribution to sudden death risk in coronary artery disease: the Oregon Sudden Unexpected Death Study. Circulation. 2009; 119:663–670.15. Goldenberg I, Moss AJ, Zareba W. QT interval: how to measure it and what is "normal". J Cardiovasc Electrophysiol. 2006; 17:333–336.16. Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983; 51:606.17. Gianrossi R, Detrano R, Mulvihill D, et al. Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation. 1989; 80:87–98.18. Aytemir K, Maarouf N, Gallagher MM, Yap YG, Waktare JE, Malik M. Comparison of formulae for heart rate correction of QT interval in exercise electrocardiograms. Pacing Clin Electrophysiol. 1999; 22:1397–1401.19. Luo S, Michler K, Johnston P, Macfarlane PW. A comparison of commonly used QT correction formulae: the effect of heart rate on the QTc of normal ECGs. J Electrocardiol. 2004; 37:Suppl. 81–90.20. Rautaharju PM, Zhang ZM. Linearly scaled, rate-invariant normal limits for QT interval: eight decades of incorrect application of power functions. J Cardiovasc Electrophysiol. 2002; 13:1211–1218.21. Chauhan VS, Krahn AD, Mitoff P, Klein GJ, Skanes AC, Yee R. Sudden intense exercise increases QT heart rate slope and T wave complexity in long QT syndrome and normal subjects. Pacing Clin Electrophysiol. 2004; 27:1415–1423.22. Kannankeril PJ, Goldberger JJ. Parasympathetic effects on cardiac electrophysiology during exercise and recovery. Am J Physiol Heart Circ Physiol. 2002; 282:H2091–H2098.23. Mittleman MA, Siscovick DS. Physical exertion as a trigger of myocardial infarction and sudden cardiac death. Cardiol Clin. 1996; 14:263–270.24. Schwartz PJ, Priori SG, Spazzolini C, et al. Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias. Circulation. 2001; 103:89–95.25. Hirao H, Shimizu W, Kurita T, et al. Frequency-dependent electrophysiologic properties of ventricular repolarization in patients with congenital long QT syndrome. J Am Coll Cardiol. 1996; 28:1269–1277.26. Shaw RM, Rudy Y. Electrophysiologic effects of acute myocardial ischemia: a theoretical study of altered cell excitability and action potential duration. Cardiovasc Res. 1997; 35:256–272.27. Lauer MS, Pothier CE, Chernyak YB, et al. Exercise-induced QT/R-R-interval hysteresis as a predictor of myocardial ischemia. J Electrocardiol. 2006; 39:315–323.28. Malik M. Problems of heart rate correction in assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol. 2001; 12:411–420.29. Magnano AR, Holleran S, Ramakrishnan R, Reiffel JA, Bloomfield DM. Autonomic nervous system influences on QT interval in normal subjects. J Am Coll Cardiol. 2002; 39:1820–1826.30. Arrowood JA, Kline J, Simpson PM, et al. Modulation of the QT interval: effects of graded exercise and reflex cardiovascular stimulation. J Appl Physiol (1985). 1993; 75:2217–2223.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of a Self Exercise Program in Cardiac Rehabilitation for Patients with Coronary Artery Disease
- Heart Rate Recovery in Coronary Artery Disease and the Changes of Exercise Parameters after Coronary Stenting
- Diagnostic Value of QT and JT Dispersion in Exercise ECG
- Study on Multistage Maximal Stress Exercise Test
- Cardiopulmonary Exercise Capacity in Coronary Artery Disease Patients Receiving Percutaneous Coronary Intervention Compared with Coronary Artery Bypass Grafting
