Obstet Gynecol Sci.
2016 Jul;59(4):286-294. 10.5468/ogs.2016.59.4.286.
Preoperative risk factors in recurrent endometrioma after primary conservative surgery
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Gil Hospital, Gachon University College of Medicine, Incheon, Korea. dongwook@gilhospital.com
- KMID: 2329049
- DOI: http://doi.org/10.5468/ogs.2016.59.4.286
Abstract
OBJECTIVE
Endometriosis is a common gynecological disorder caused by ectopic implantation of endometrial glandular and stromal cells outside the uterine cavity. Among several types of endometriosis, endometrioma is the only subtype that could be determined preoperatively using pelvic ultrasonography, and guidelines recommend pathologic confirmation of endometrioma greater than 3 cm in diameter. However, although surgery is performed in cases of endometrioma, endometrioma has a high cumulative rate of recurrence. Therefore, because determining the possibility of recurrence before performance of initial surgery is important, we examined preoperative factors associated with recurrent endometrioma.
METHODS
This was a retrospective, comparative study including 236 patients who visited the outpatient clinic between January 2009 and December 2011. Patients who were pathologically diagnosed with endometrioma were included in this study. They were followed up postoperatively and were divided into two groups according to presence of recurrent endometrioma.
RESULTS
We examined associations between baseline factors and recurrent endometrioma. In multivariate analysis, dysmenorrhea and cyst septation were statistically significant after adjusting with age, parity, surgical staging and postoperative management. We examined cumulative recurrence free survival within cases of recurrent endometriosis, based on the presence of inner cyst septation. The cumulative recurrence free survival was lower in cases with septation.
CONCLUSION
Our study found that recurrent endometrioma is more likely in patients with inner cyst septation and the recurrence occurred within a shorter duration of time than in patients without inner cyst septation on preoperative ultrasonography. Therefore intensive caution and postoperative long term medical therapy would be appropriate in patients with inner cyst septation on preoperative ultrasonography before undergoing primary surgery for endometrioma.
Keyword
MeSH Terms
Figure
-
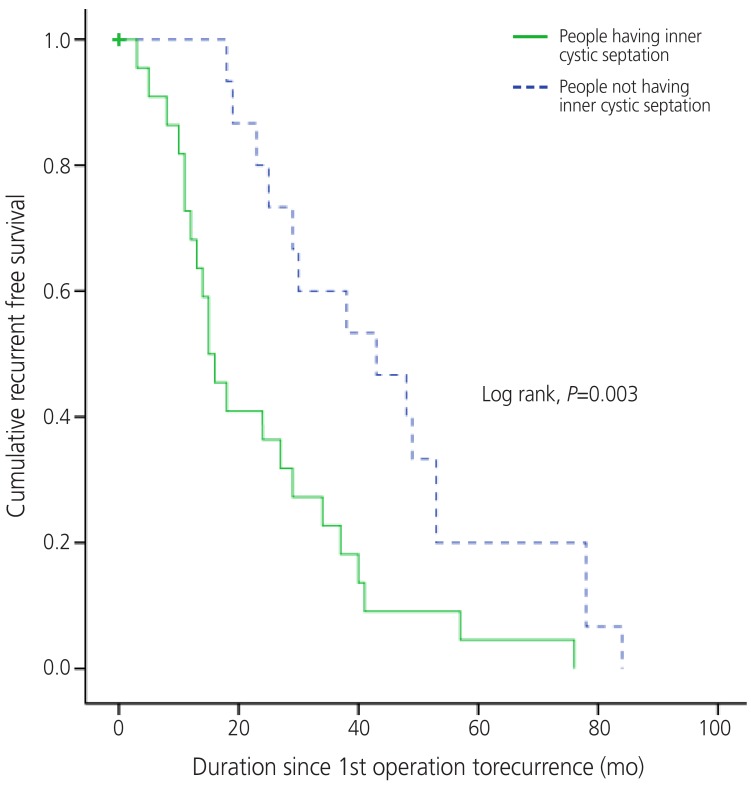
Fig. 1 Cumulative recurrent free survival according to presence of septation within endometrioma in cases with recurrent endometrioma. People having inner cystic septation was associated with recurrence within shorter period of time (log rank, P=0.003) than people without septation.
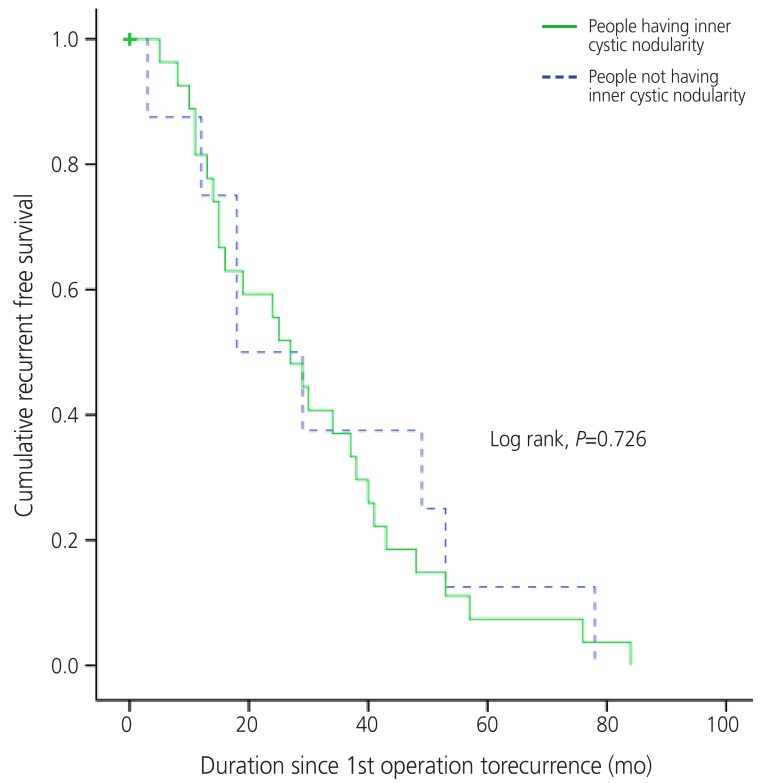
Fig. 2 Cumulative recurrent free survival according to presence of nodularity within endometrioma in cases with recurrent endometrioma. People with and without inner cystic nodularity had no difference in duration of recurrence since 1st operation (log rank, P=0.726).
Reference
-
3. Kennedy S, Bergqvist A, Chapron C, D'Hooghe T, Dunselman G, Greb R, et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod. 2005; 20:2698–2704. PMID: 15980014.
Article4. Nisolle M, Donnez J. Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil Steril. 1997; 68:585–596. PMID: 9341595.
Article5. Busacca M, Marana R, Caruana P, Candiani M, Muzii L, Calia C, et al. Recurrence of ovarian endometrioma after laparoscopic excision. Am J Obstet Gynecol. 1999; 180(3 Pt 1):519–23. PMID: 10076121.
Article6. Koga K, Takemura Y, Osuga Y, Yoshino O, Hirota Y, Hirata T, et al. Recurrence of ovarian endometrioma after laparoscopic excision. Hum Reprod. 2006; 21:2171–2174. PMID: 16644912.
Article7. Jones KD, Sutton CJ. Recurrence of chocolate cysts after laparoscopic ablation. J Am Assoc Gynecol Laparosc. 2002; 9:315–320. PMID: 12101328.
Article8. Kikuchi I, Takeuchi H, Kitade M, Shimanuki H, Kumakiri J, Kinoshita K. Recurrence rate of endometriomas following a laparoscopic cystectomy. Acta Obstet Gynecol Scand. 2006; 85:1120–1124. PMID: 16929419.
Article9. Liu X, Yuan L, Shen F, Zhu Z, Jiang H, Guo SW. Patterns of and risk factors for recurrence in women with ovarian endometriomas. Obstet Gynecol. 2007; 109:1411–1420. PMID: 17540815.
Article10. Hayasaka S, Ugajin T, Fujii O, Nabeshima H, Utsunomiya H, Yokomizo R, et al. Risk factors for recurrence and rerecurrence of ovarian endometriomas after laparoscopic excision. J Obstet Gynaecol Res. 2011; 37:581–585. PMID: 21159045.
Article11. Yun BH, Jeon YE, Chon SJ, Park JH, Seo SK, Cho S, et al. The prognostic value of individual adhesion scores from the revised American Fertility Society classification system for recurrent endometriosis. Yonsei Med J. 2015; 56:1079–1086. PMID: 26069133.
Article12. Tosti C, Pinzauti S, Santulli P, Chapron C, Petraglia F. Pathogenetic mechanisms of deep infiltrating endometriosis. Reprod Sci. 2015; 22:1053–1059. PMID: 26169038.
Article13. Lee DY, Kim HJ, Yoon BK, Choi D. Factors associated with the laterality of recurrent endometriomas after conservative surgery. Gynecol Endocrinol. 2013; 29:978–981. PMID: 24004294.
Article14. Vercellini P, Aimi G, De Giorgi O, Maddalena S, Carinelli S, Crosignani PG. Is cystic ovarian endometriosis an asymmetric disease? Br J Obstet Gynaecol. 1998; 105:1018–1021. PMID: 9763055.
Article15. Parazzini F. Left:right side ratio of endometriotic implants in the pelvis. Eur J Obstet Gynecol Reprod Biol. 2003; 111:65–67. PMID: 14557014.
Article16. Al-Fozan H, Tulandi T. Left lateral predisposition of endometriosis and endometrioma. Obstet Gynecol. 2003; 101:164–166. PMID: 12517662.
Article17. Matalliotakis IM, Cakmak H, Koumantakis EE, Margariti A, Neonaki M, Goumenou AG. Arguments for a left lateral predisposition of endometrioma. Fertil Steril. 2009; 91:975–978. PMID: 18353324.
Article18. Bricou A, Batt RE, Chapron C. Peritoneal fluid flow influences anatomical distribution of endometriotic lesions: why Sampson seems to be right. Eur J Obstet Gynecol Reprod Biol. 2008; 138:127–134. PMID: 18336988.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of Post-Operative Medication to Prevent Recurrence of Endometrioma: Cyclic Oral Contraceptive (OC) After Gonadotropin-Releasing Hormone (GnRH) Agonist Versus Dienogest
- Effect of second-line surgery on in vitro fertilization outcome in infertile women with ovarian endometrioma recurrence after primary conservative surgery for moderate to severe endometriosis
- Assessment of Ovarian Volume and Hormonal Changes after Ovarian Cystectomy in the Different Ovarian Tumor
- A Case of Pelviscopic Surgery for Huge Endometrioma
- Recurrence, Reoperation, Pregnancy Rates, and Risk Factors for Recurrence after Ovarian Endometrioma Surgery: Long-Term Follow-Up of 756 Women
