J Dent Anesth Pain Med.
2016 Jun;16(2):141-145. 10.17245/jdapm.2016.16.2.141.
Occurrence of bilateral pneumothorax during tracheostomy in a patient with deep neck infection
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea.
- 2Department of Otorhinolaryngology, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea. manbang5@naver.com
- KMID: 2328858
- DOI: http://doi.org/10.17245/jdapm.2016.16.2.141
Abstract
- Infection that progresses to deep areas of the neck requires appropriate assessment of the airway, and securing of the airway is critical in patients with deep neck infection. In the patient in our case report, bilateral pneumothorax occurred while performing tracheostomy to the airways of a patient with deep neck infection, and therefore, this paper details the method used to secure the airway of patients with deep neck infection.
Keyword
MeSH Terms
Figure
-
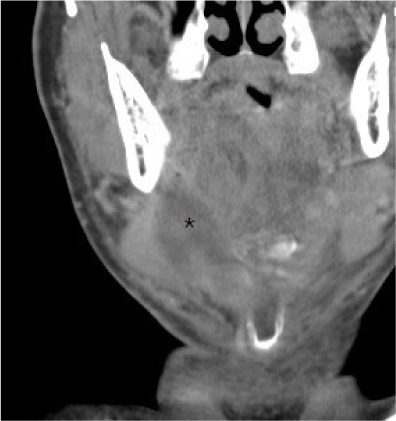
Fig. 1 Submandibular space abscess (star) on computed tomography (CT) imaging acquired in the emergency room. Neck CT coronal view.

Fig. 2 Image of airway evaluation acquired in the emergency room. Neck CT sagittal view.

Fig. 3 The right-sided pneumothorax appearing on the chest anteroposterior (AP) radiograph acquired after tracheostomy.
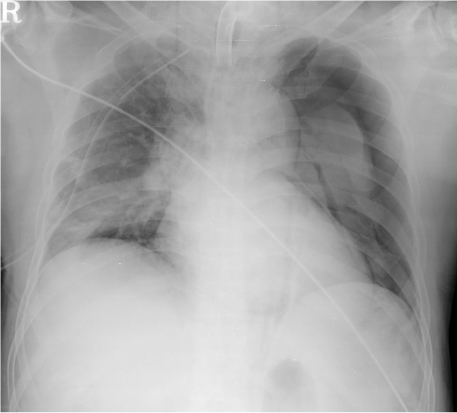
Fig. 4 The pneumothorax additionally found in the left lung area on a chest AP radiograph taken in the ICU following thoracentesis using a chest tube in the right lung area previously.

Fig. 5 The bilaterally reduced pneumothorax as seen on the chest radiograph taken following bilateral thoracentesis using a chest tube in the bilateral lung area.
Reference
-
1. Karkos PD, Leong SC, Beer H, Apostolidou MT, Panarese A. Challenging airways in deep neck space infections. Am J Otolaryngol. 2007; 28:415–418.
Article2. Chen SJ, Ji N, Chen YX, Zhao SJ, Xiao JR, Lin XM, et al. Management and maintenance of the airway in cervical necrotising fasciitis: a retrospective analysis of 15 cases. Br J Oral Maxillofac Surg. 2015; 53:642–646.3. Kumar D, O'Hare B, Timon C, Mukhtar M, Kelly D. Bilateral pneumothoraces and pulmonary oedema following tracheostomy induced by acute tracheal obstruction. BMJ Case Rep. 2012; 2012.4. Pappachan B. Acute airway distress secondary to iatrogenic injury during Tracheostomy. J Maxillofac Oral Surg. 2009; 8:91–93.
Article5. Yoo H, Choi JM, Jo JY, Lee S, Jeong SM. Blind nasal intubation as an alternative to difficult intubation approaches. J Dent Anesth Pain Med. 2015; 15:181.
Article6. Moon YJ, Kim J, Seo DW, Kim JW, Jung HW, Suk EH, et al. Endotracheal intubation by inexperienced trainees using the Clarus Video System: learning curve and orodental trauma perspectives. J Dent Anesth Pain Med. 2015; 1:207.
Article7. Giordano D, Panini A, Pernice C, Raso MG, Barbieri V. Neurologic toxicity of lidocaine during awake intubation in a patient with tongue base abscess. Case report. Am J Otolaryngol. 2014; 35:62–65.
Article8. Wolfe MM, Davis JW, Parks SN. Is surgical airway necessary for airway management in deep neck infections and Ludwig angina? J Crit Care. 2011; 26:11–14.
Article9. Fichtner A, Vrtny P, Schaarschmidt F. [Ultrasound-guided retrograde emergency intubation : Life-saving management of a bleeding airway emergency with unclear anatomical situation]. Anaesthesist. 2015; DOI: 10.1007/s00101-015-0102-y.
Article10. Kim JS, Seo DK, Lee CJ, Jung HS, Kim SS. Difficult intubation using intubating laryngeal mask airway in conjunction with a fiber optic bronchoscope. J Dent Anesth Pain Med. 2015; 15:167.11. Kim WH, Kim BH. Bilateral pneumothoraces, pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema after percutaneous tracheostomy -A case report. Korean J Anesthesiol. 2012; 62:488–492.12. Lodhia JV, Ismail I, Christensen TD. Bilateral pneumothoraces in a patient with laryngeal carcinoma following tracheostomy for stridor. BMJ Case Rep. 2014; 2:2014.
Article13. Kundranda RM, Trochtenberg DS. Bilateral pneumothorax as a complication of changing tracheostomy tube. Tenn Med. 2003; 96:225–226.
Article14. Teo N, Garrahy A. Elective surgical cricothyroidotomy in oral and maxillofacial surgery. Br J Oral Maxillofac Surg. 2013; 51:779–782.
Article15. Fang CH, Friedman R, White PE, Mady LJ, Kalyoussef E. Emergent Awake tracheostomy-The five-year experience at an urban tertiary care center. Laryngoscope. 2015; 125:2476–2479.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Tracheostomy Induced Bilateral Tension Pneumothorax
- A Case of Pneumothorax and Subcutaneous Emphysema in a Tracheostomized Patient during General Anesthesia
- Bilateral pneumothoraces, pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema after percutaneous tracheostomy: A case report
- Life-threatening tension pneumothorax after unsuccessful tracheostomy tube exchange in a trauma patient - A case report -
- Simultaneous Bilateral Spontaneous Pneumothorax
