J Lipid Atheroscler.
2016 Jun;5(1):93-97. 10.12997/jla.2016.5.1.93.
A Case of Bilateral Renal Infarction of Unknown Cause in a Previously Healthy Young Male
- Affiliations
-
- 1Department of Internal Medicine, Myongji Hospital, Seonam University School of Medicine, Goyang, Gyeonggi-do, Korea. ltriver@hanmail.net
- KMID: 2328842
- DOI: http://doi.org/10.12997/jla.2016.5.1.93
Abstract
- We report a rare case of bilateral renal infarction resulting in acute renal failure in a previously healthy 26-year-old soldier. The patient presented with an abdominal pain and bilateral costovertebral angle tenderness. Laboratory studies showed elevated serum creatinine, mild leukocytosis, and increased lactate dehydrogenase. Contrast-enhanced computed tomography showed multiple perfusion defects in both kidneys with wedge-shaped infarction in right kidney. Kidney biopsy performed in the left kidney revealed microinfarction. Comprehensive work-up did not reveal any specific causes or risk factors except smoking, and the infarction was considered to be idiopathic. He emphasized that he received extremely strenuous military training several days before he came to the hospital. He was treated with low molecular weight heparin with significant improvement in renal function. Further studies are needed for the characterization of idiopathic renal infarction in previously healthy individuals and evaluating the mechanisms including strenuous physical activity on the renal blood flow.
MeSH Terms
Figure
-
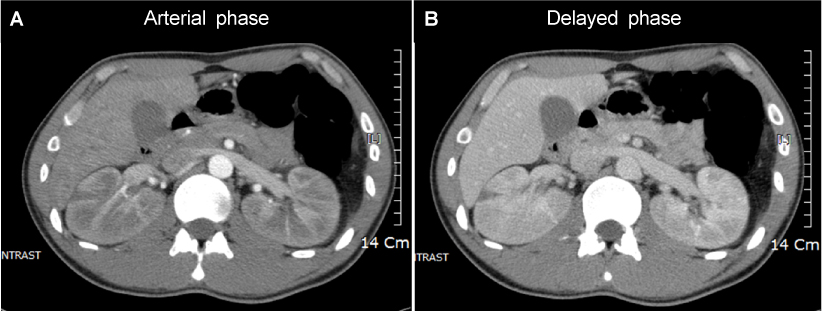
Fig. 1 Contrast-enhanced abdominal computed tomography (CT). (A) Arterial phase, (B) Delayed phase, CT demonstrated mild enlargement, multiple perfusion defects and delayed contrast excretion in bilateral kidneys with unequivocal wedge-shaped infarction in right kidney.
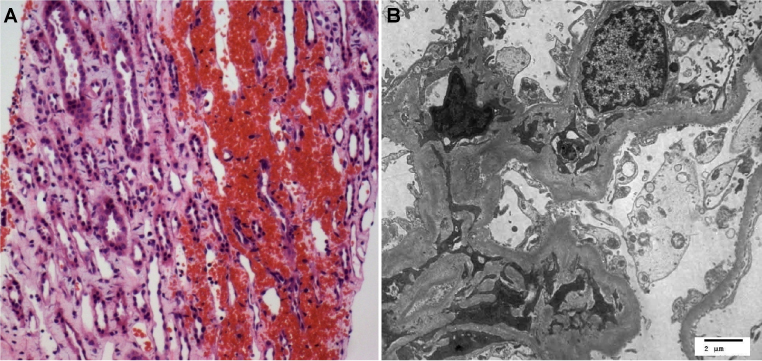
Fig. 2 Renal biopsy findings. (A) Light microscopy (×10). In the renal cortex, patch microinfarction is shown with loss of nuclei and ballooning degeneration of tubular epithelial cells (not shown). In the medulla, severe interstitial hemorrhage is also shown, (B) Transmission electron microscopy (TEM) (×5000). Ultrastructurely, glomerular cells, particularly podocytes, exhibit severe necrosis, entirely detached from the glomerular basement membrane.
Reference
-
1. Korzets Z, Plotkin E, Bernheim J, Zissin R. The clinical spectrum of acute renal infarction. Isr Med Assoc J. 2002; 4:781–784.2. Antopolsky M, Simanovsky N, Stalnikowicz R, Salameh S, Hiller N. Renal infarction in the ED: 10-year experience and review of the literature. Am J Emerg Med. 2012; 30:1055–1060.
Article3. Bourgault M, Grimbert P, Verret C, Pourrat J, Herody M, Halimi JM, et al. Acute renal infarction: a case series. Clin J Am Soc Nephrol. 2013; 8:392–398.
Article4. Racusin JS, Pollack ML. Idiopathic renal infarction in a young woman. Am J Emerg Med. 2005; 23:397–398.
Article5. Joulin V, Sallusto F, Deruelle C, Taccoen X, Valeri A, Fournier G. Idiopathic acute partial renal infarction. Prog Urol. 2005; 15:75–77.6. Eickhoff C, Mei JM, Martinez J, Little D. Idiopathic renal infarction in a previously healthy active duty soldier. Mil Med. 2014; 179:e259–e262.
Article7. Tsai SH, Chu SJ, Chen SJ, Fan YM, Chang WC, Wu CP, et al. Acute renal infarction: a 10-year experience. Int J Clin Pract. 2007; 61:62–67.
Article8. Paris B, Bobrie G, Rossignol P, Le Coz S, Chedid A, Plouin PF. Blood pressure and renal outcomes in patients with kidney infarction and hypertension. J Hypertens. 2006; 24:1649–1654.
Article9. Manfredini R, La Cecilia O, Ughi G, Kuwornu H, Bressan S, Regoli F, et al. Renal infarction: an uncommon mimic presenting with flank pain. Am J Emerg Med. 2000; 18:325–327.
Article10. Yen TH, Chang CT, Ng KK, Wu MS. Bilateral renal infarction in chronic myelomonocytic leukemia on blast crisis. Ren Fail. 2003; 25:1029–1035.
Article11. Bouassida K, Hmida W, Zairi A, Hidoussi A, Jaidane M, Slama A, et al. Bilateral renal infarction following atrial fibrillation and thromboembolism and presenting as acute abdominal pain: a case report. J Med Case Rep. 2012; 6:153.
Article12. Padilla-Fernández B, García-Casado D, Martín-Izquierdo M, Manzano-Rodríguez C, García-García J, Lorenzo-Gómez MF. Bilateral renal infarction in a lupus patient: an unusual pathology. Clin Med Insights Case Rep. 2013; 6:87–91.
Article13. González-Moreno J, Campins MA, Buades JM. Fibromuscular dysplasia presenting with asymptomatic bilateral renal infarctions. Int Urol Nephrol. 2014; 46:243–246.
Article14. Bolderman R, Oyen R, Verrijcken A, Knockaert D, Vanderschueren S. Idiopathic renal infarction. Am J Med. 2006; 119:356.e9–356.e12.
Article15. Huang CC, Lo HC, Huang HH, Kao WF, Yen DH, Wang LM, et al. ED presentations of acute renal infarction. Am J Emerg Med. 2007; 25:164–169.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Spontaneous Renal Artery Dissection Causing Renal Infarction in a Previously Healthy Man
- Spontaneous Renal Artery Dissection Complicated by Renal Infarction: Three Case Reports
- A Case of Recurrent Renal Infarction Due to Fibromuscula Dysplasia
- Two Cases of Spontaneous Renal Artery Dissection: Diagnosis using Abdominal Computed Tomography
- A Case of Idipathic Bilateral Renal and Splenic Infarctions in a Healthy Man
