Evaluation of augmented alveolar bone with vertical alveolar distraction osteogenesis and implant installation
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Chonnam National University, Gwangju, Korea. hkoh@jnu.ac.kr
Abstract
- INTRODUCTION
The purpose of this study was to evaluate the clinical result of vertical alveolar distraction, especially the distracted alveolar bone and installed implants.
MATERIALS AND METHODS
Twenty-one patients who have been received the vertical alveolar distraction and implant installation on 22 areas (3 maxilla and 19 mandible) using intraoral alveolar distraction device were examined. After consolidation period of 3-4 months, distraction devices were removed and 91 implants were installed in the distracted alveolar bone. The distracted bone and implants were evaluated clinically and radiographically.
RESULTS
Mean height of distracted alveolar bone was 7.5+/-3.2 mm (range: 2.5-15.0 mm). Mean follow-up period after completion of the distraction was 3.1 years (range: 1.4-11.5 years). Mean resorption of distracted alveolar bone was 1.6+/-1.8 mm. The success and survival rates of implants was 95.3% and 100%, respectively.
CONCLUSION
Results of this study indicate that vertical alveolar distraction procedure is a useful and stable method for alveolar ridge augmentation and implantation.
Keyword
MeSH Terms
Figure
-
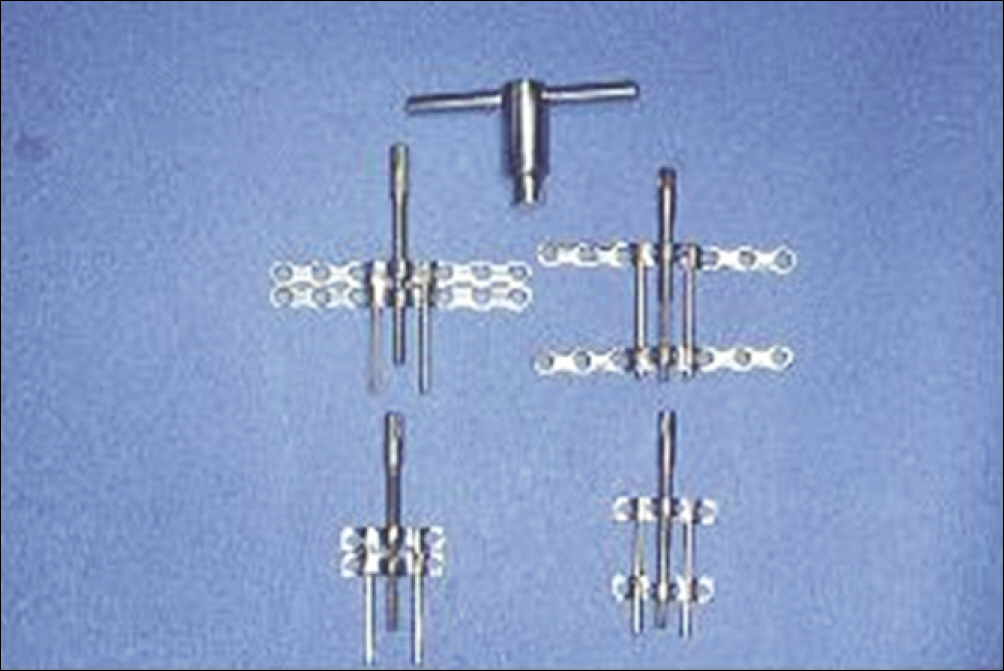
Fig. 1. Intraoral vertical alveolar distractor. Uttom Kumar Shet et al: Evaluation of augmented alveolar bone with vertical alveolar distraction osteogenesis and implant installation. J Korean Assoc Oral Maxillofac Surg 2011

Fig. 2. Panoramic radiographs of the patient who underwent alveolar bone distraction osteogenesis (ABDO) after marginal mandibulectomy. A: Before the ABDO, B: Immediate after the ABDO, C: After the ABDO, just before the device removal and implant installation, D: Implant installation. postoperative six months (from the distraction osteogenesis device application), E: Completion of the prothodontic treatment. postoperative one year, F: postoperative eight years four months. Uttom Kumar Shet et al: Evaluation of augmented alveolar bone with vertical alveolar distraction osteogenesis and implant installation. J Korean Assoc Oral Maxillofac Surg 2011
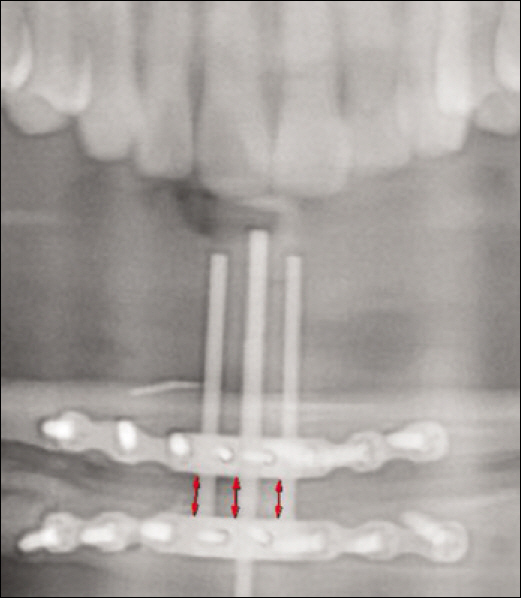
Fig. 3. Measuring of the gained bone height. Uttom Kumar Shet et al: Evaluation of augmented alveolar bone with vertical alveolar distraction osteogenesis and implant installation. J Korean Assoc Oral Maxillofac Surg 2011
Reference
-
References
1. Keller EE, Triplett WW. Iliac bone grafting: review of 160 consecutive cases. J Oral Maxillofac Surg. 1987; 45:11–4.
Article2. Costantino PD, Shybut G, Friedman CD, Pelzer HJ, Masini M, Shindo ML, et al. Segmental mandibular regeneration by distraction osteogenesis. An experimental study. Arch Otolaryngol Head Neck Surg. 1990; 116:535–45.
Article3. Codivilla A. On the means of lengthening in the lower limbs, the musles, and tissues which are shortened through deformity. J Bone Joint Surg Am. 1905; s2–2:353–69.4. Ilizarov GA. The principles of the Ilizarov method. Bull Hosp Jt Dis Orthop Inst. 1988; 48:1–11.5. McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992; 89:1–8. discussion 9–10.
Article6. Nishimura T, Jinbo M, Ikeda H, Masahiko S, Nara S, Toriyabe M, et al. Study on ridge augmentation by callus distraction (cal-lotasis). Jpn J Oral Maxillofac Surg. 1992; 38:1357–63.
Article7. Chin M, Toth BA. Distraction osteogenesis in maxillofacial surgery using internal devices: review of five cases. J Oral Maxillofac Surg. 1996; 54:45–53. discussion 54.
Article8. Buser D, Mericske-Stern R, Bernard JP, Behneke A, Behneke N, Hirt HP, et al. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multicenter study with 2359 implants. Clin Oral Implants Res. 1997; 8:161–72.
Article9. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The longterm efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986; 1:11–25.10. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res. 1989. 263–85.11. Kojimoto H, Yasui N, Goto T, Matsuda S, Shimomura Y. Bone lengthening in rabbits by callus distraction. The role of periosteum and endosteum. J Bone Joint Surg Br. 1988; 70:543–9.
Article12. Lee YU, Park CY, Song JW, Park HJ, Kim YW, Oh HK, et al. Implant installation after mandibular alveolar ridge augmentation using intraoral distraction device: report of 5 cases. J Korean Assoc Maxillofac Plast Reconstr Surg. 2002; 24:176–83.13. Chiapasco M, Consolo U, Bianchi A, Ronchi P. Alveolar distraction osteogenesis for the correction of vertically deficient edentulous ridges: a multicenter prospective study on humans. Int J Oral Maxillofac Implants. 2004; 19:399–407.
Article14. Enislidis G, Fock N, Millesi-Schobel G, Klug C, Wittwer G, Yerit K, et al. Analysis of complications following alveolar distraction osteogenesis and implant placement in the partially edentulous mandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:25–30.
Article15. Ettl T, Gerlach T, Schu ¨sselbauer T, Gosau M, Reichert TE, Driemel O. Bone resorption and complications in alveolar distraction osteogenesis. Clin Oral Investig. 2010; 14:481–9.
Article16. Block MS, Cervini D, Chang A, Gottsegen GB. Anterior maxillary advancement using tooth-supported distraction osteogenesis. J Oral Maxillofac Surg. 1995; 53:561–5.
Article17. Rachmiel A, Levy M, Laufer D. Lengthening of the mandible by distraction osteogenesis: report of cases. J Oral Maxillofac Surg. 1995; 53:838–46.18. Garcia AG, Martin MS, Vila PG, Maceiras JL. Minor complications arising in alveolar distraction osteogenesis. J Oral Maxillofac Surg. 2002; 60:496–501.
Article19. Snyder CC, Levine GA, Swanson HM, Browne EZ Jr. Mandibular lengthening by gradual distraction. Preliminary report. Plast Reconstr Surg. 1973; 51:506–8.20. Block MS, Daire J, Stover J, Matthews M. Changes in the inferior alveolar nerve following mandibular lengthening in the dog using distraction osteogenesis. J Oral Maxillofac Surg. 1993; 51:652–60.
Article21. Gantous A, Phillips JH, Catton P, Holmberg D. Distraction osteogenesis in the irradiated canine mandible. Plast Reconstr Surg. 1994; 93:164–8.
Article22. Uckan S, Haydar SG, Dolanmaz D. Alveolar distraction: analysis of 10 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:561–5.
Article23. Chiapasco M, Romeo E, Vogel G. Vertical distraction osteogenesis of edentulous ridges for improvement of oral implant positioning: a clinical report of preliminary results. Int J Oral Maxillofac Implants. 2001; 16:43–51.24. Mazzonetto R, Allais M, Maurette PE, Moreira RW. A retrospective study of the potential complications during alveolar distraction osteogenesis in 55 patients. Int J Oral Maxillofac Surg. 2007; 36:6–10.
Article25. Uckan S, Haydar SG, Imirzalioglu P, Acar AG. Repositioning of malpositioned segment during alveolar distraction. J Oral Maxillofac Surg. 2002; 60:963–5.
Article26. Oh HK, Park HJ, Cho JY, Park YJ, Kook MS. Vector control of malpositioned segment during alveolar distraction osteogenesis by using rubber traction. J Oral Maxillofac Surg. 2009; 67:608–12.
Article27. Erkut S, Uckan S. Alveolar distraction osteogenesis and implant placement in a severely resorbed maxilla: a clinical report. J Prosthet Dent. 2006; 95:340–3.
Article28. Kilic E, Kilic K, Alkan A. Alternative method to reposition the dislocated transport segment during vertical alveolar distraction. J Oral Maxillofac Surg. 2009; 67:2306–10.
Article29. Mazzonetto R, Serra E Silva FM, Ribeiro Torezan JF. Clinical assessment of 40 patients subjected to alveolar distraction osteogenesis. Implant Dent. 2005; 14:149–53.
Article30. Paeng JY, Myoung H, Hwang SJ, Seo BM, Choi JY, Lee JH, et al. Clinical evaluation of alveolar distraction osteogenesis for implant installation. J Korean Assoc Maxillofac Plast Reconstr Surg. 2006; 28:329–38.31. Garcia AG, Martin MS, Vila PG, Saulacic N, Rey JM. Palatal approach for maxillary alveolar distraction. J Oral Maxillofac Surg. 2004; 62:795–8.
Article32. Jensen OT, Cockrell R, Kuhike L, Reed C. Anterior maxillary alveolar distraction osteogenesis: a prospective 5-year clinical study. Int J Oral Maxillofac Implants. 2002; 17:52–68.33. Saulacic′N. Somosa Martl′n M, de Los Angeles Leon Camacho M, Garcl′a Garcl′a A. Complications in alveolar distraction osteogenesis: A clinical investigation. J Oral Maxillofac Surg. 2007; 65:267–74.34. Block MS, Almerico B, Crawford C, Gardiner D, Chang A. Bone response to functioning implants in dog mandibular alveolar ridges augmented with distraction osteogenesis. Int J Oral Maxillofac Implants. 1998; 13:342–51.35. Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants. 2007; 22(Suppl):49–70.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical evaluation of alveolar distraction osteogenesis for implant installation
- Vertical Distraction Of Alveolar Bone For Placement Of Dental Implant
- Dental implant treatment with iliac bone graft via two-stage approach for avulsed alveolar bone defects; case report
- A case report of implant placement in distraction-augmented alveolar bone of the mandible
- Solutions and Prevention of Problems Arising from Alveolar Distraction Osteogenesis: 4 Case Reports
