A clinical study of iliac bone graft using subperiosteal tunneling method for alveolar ridge augmentation
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyunghee University, Seoul, Korea. leebs@khu.ac.kr
Abstract
- PURPOSE
The objective of this study was to evaluate the efficacy of the subperiosteal tunneling technique with iliac block bone graft for bone augmentation in an edentulous alveolar ridge.
PATIENTS AND METHODS
Total of 8 sites in 7 patients were included in this study. The bone height was evaluated by CBCT preoperatively and 4 months after operation. Total of 11 implants were inserted and evaluated clinically and radiographically.
RESULTS
Mean value of the increased bone height was 6.29 mm and no implant failure was observed. There were no complications such as soft tissue dehiscence, exposure of the grafted bone and infection.
CONCLUSION
We have achieved excellent clinical outcomes by this technique, so we concluded that it is useful for augmentation of severely deficient alveolar ridge.
Figure
-
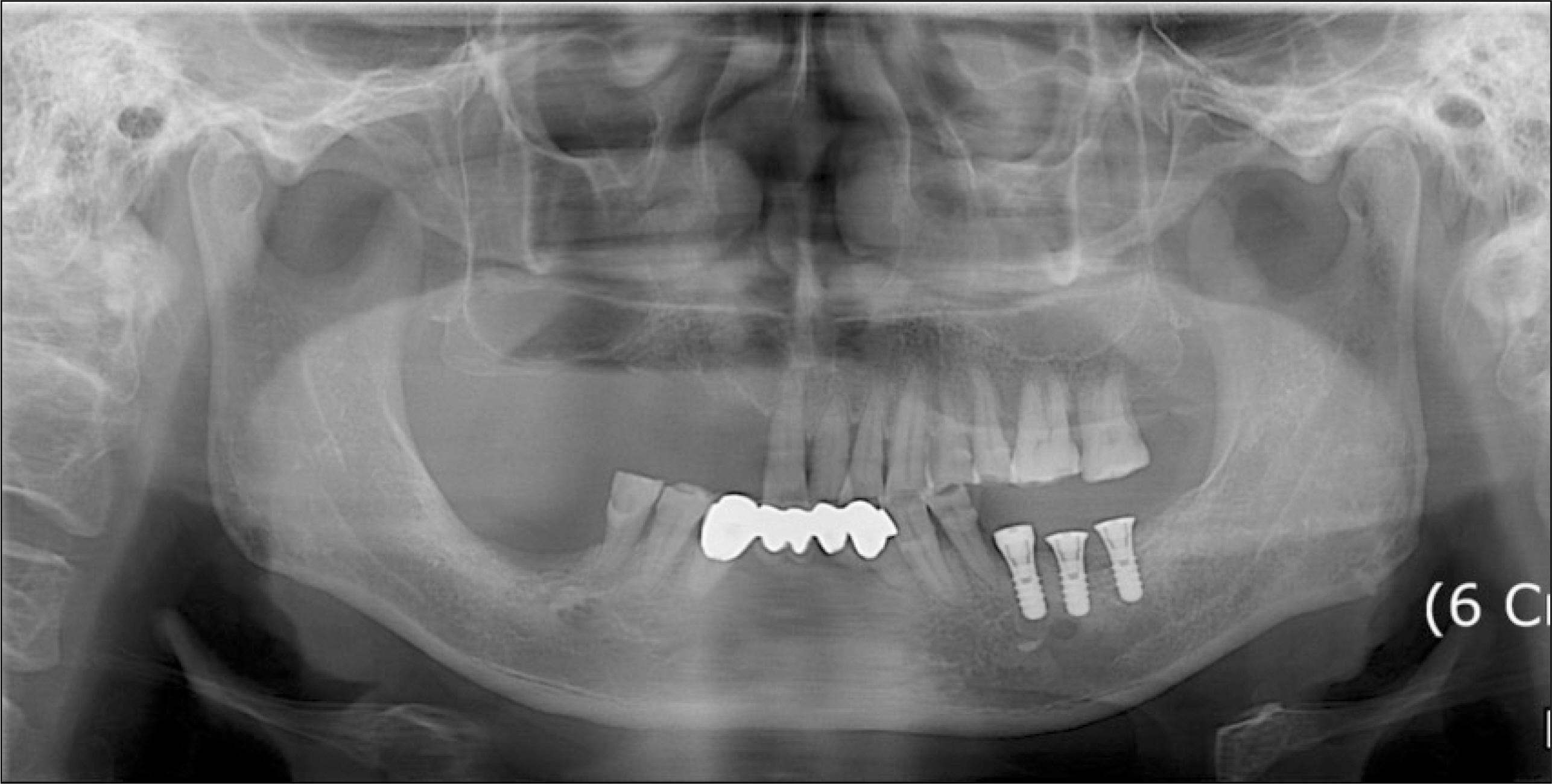
Fig. 1. Preoperative panoramic view showing atrophic ridge on right edentulous mandibular molar area.

Fig. 2. Clinical photo of deficient right mandibular alveolar ridge.
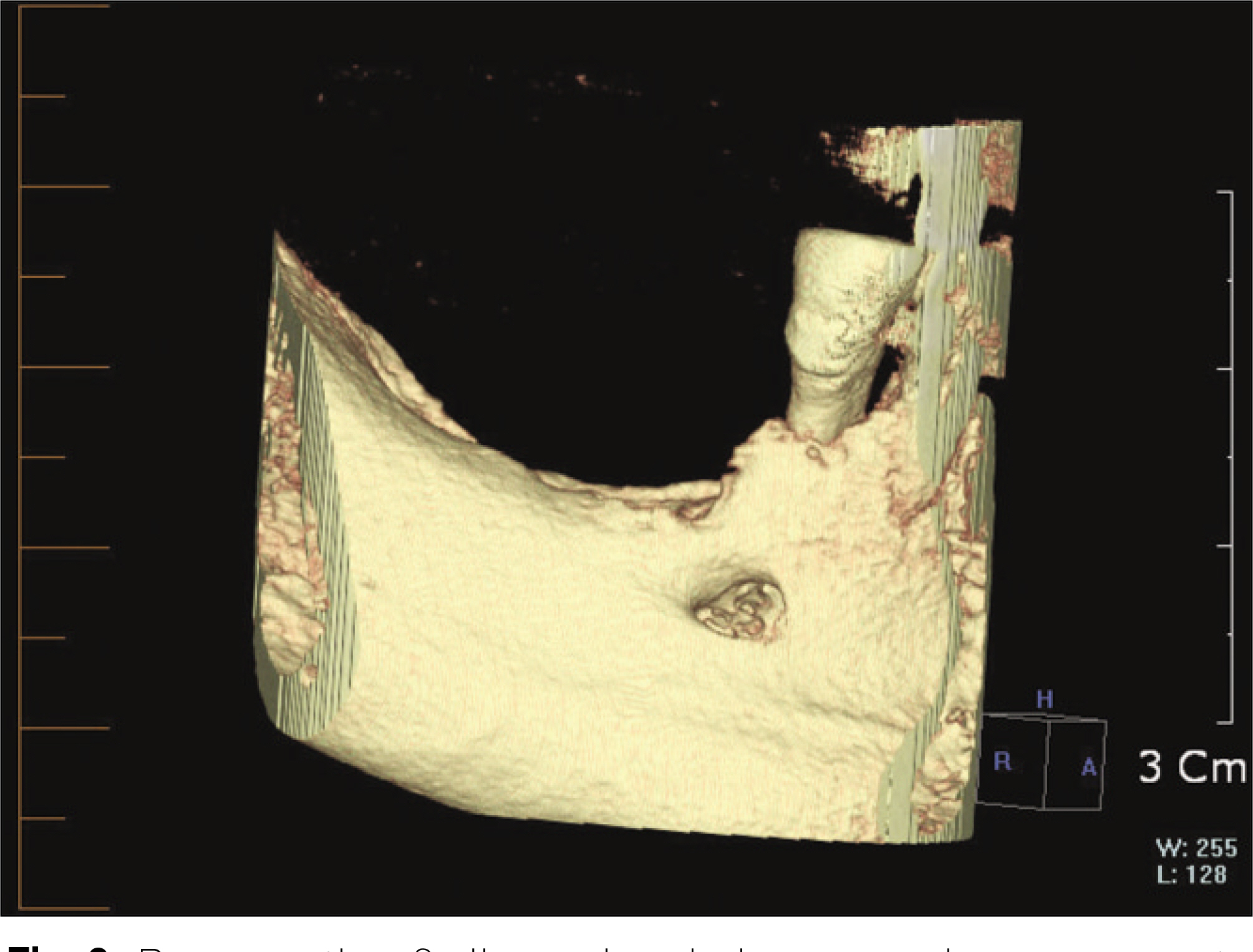
Fig. 3. Preoperative 3 dimensional view conebeam computerized tomography (CBCT) scan showing the right mandibular alveolar ridge.
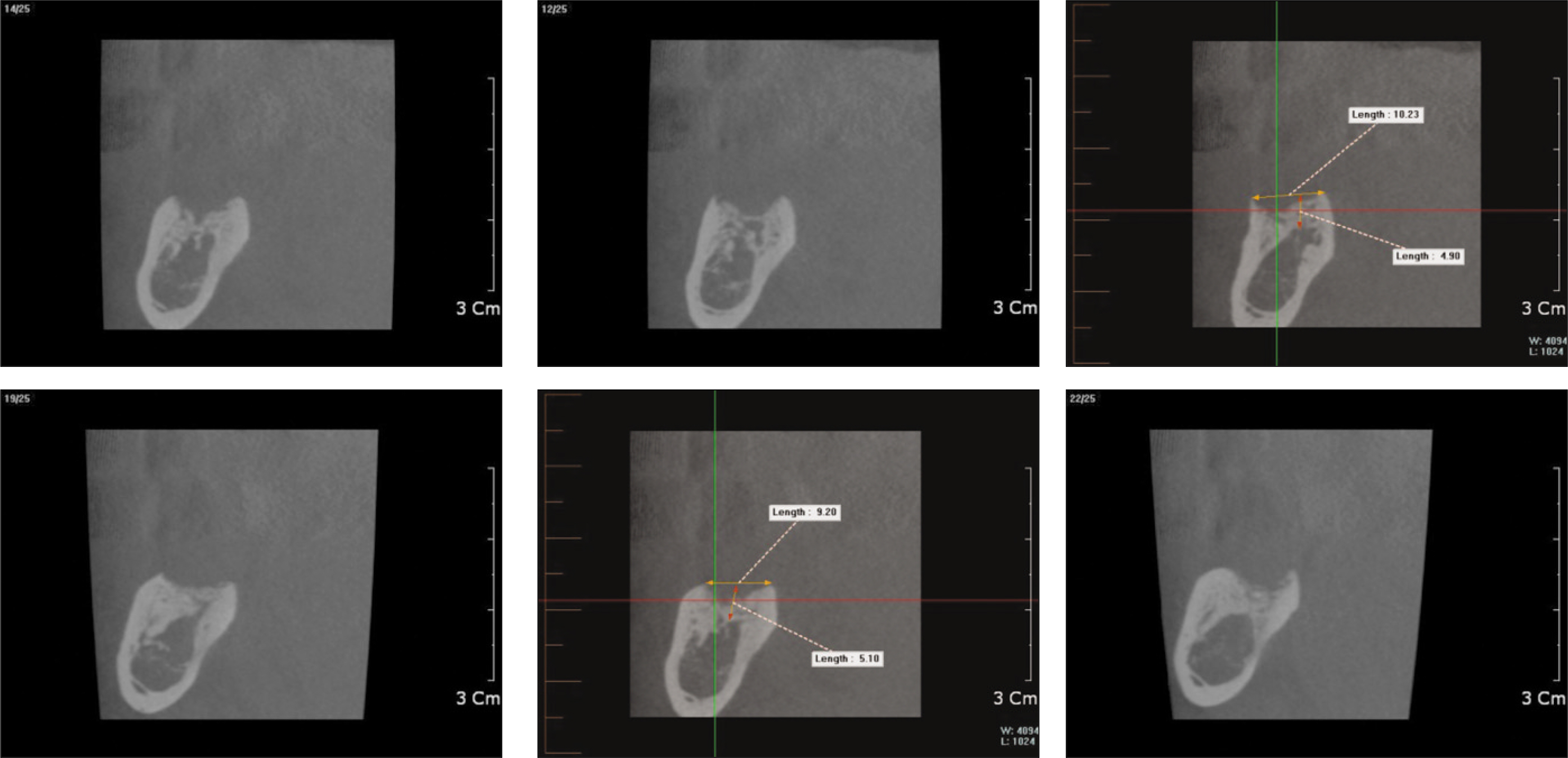
Fig. 4. Computed tomography (CT) scan showing deficient area before iliac bone graft. It shows close approximation to inferior alveolar nerve due to severe vertical alveolar bone resorption.
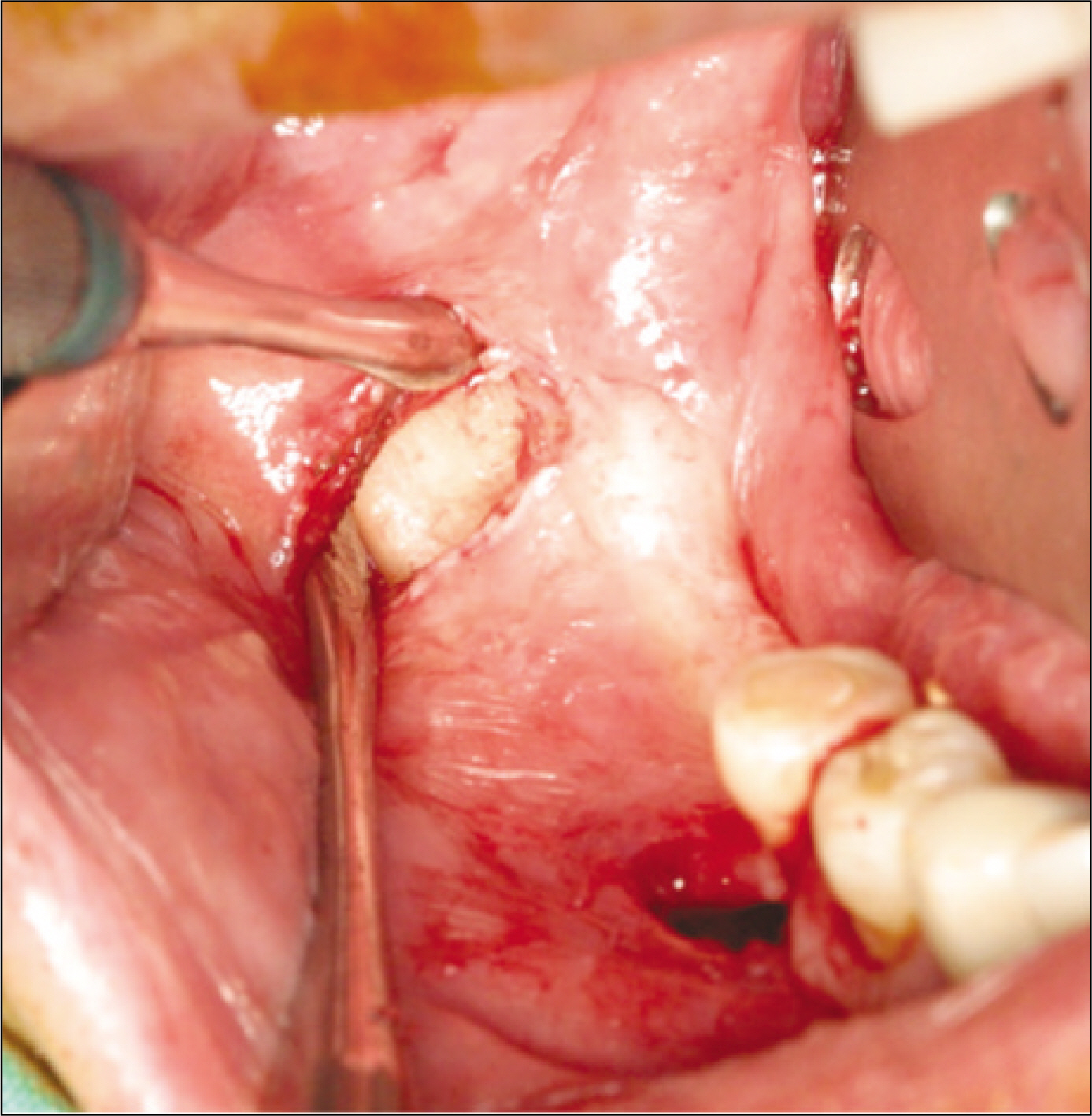
Fig. 5. Two vertical incisions are made.
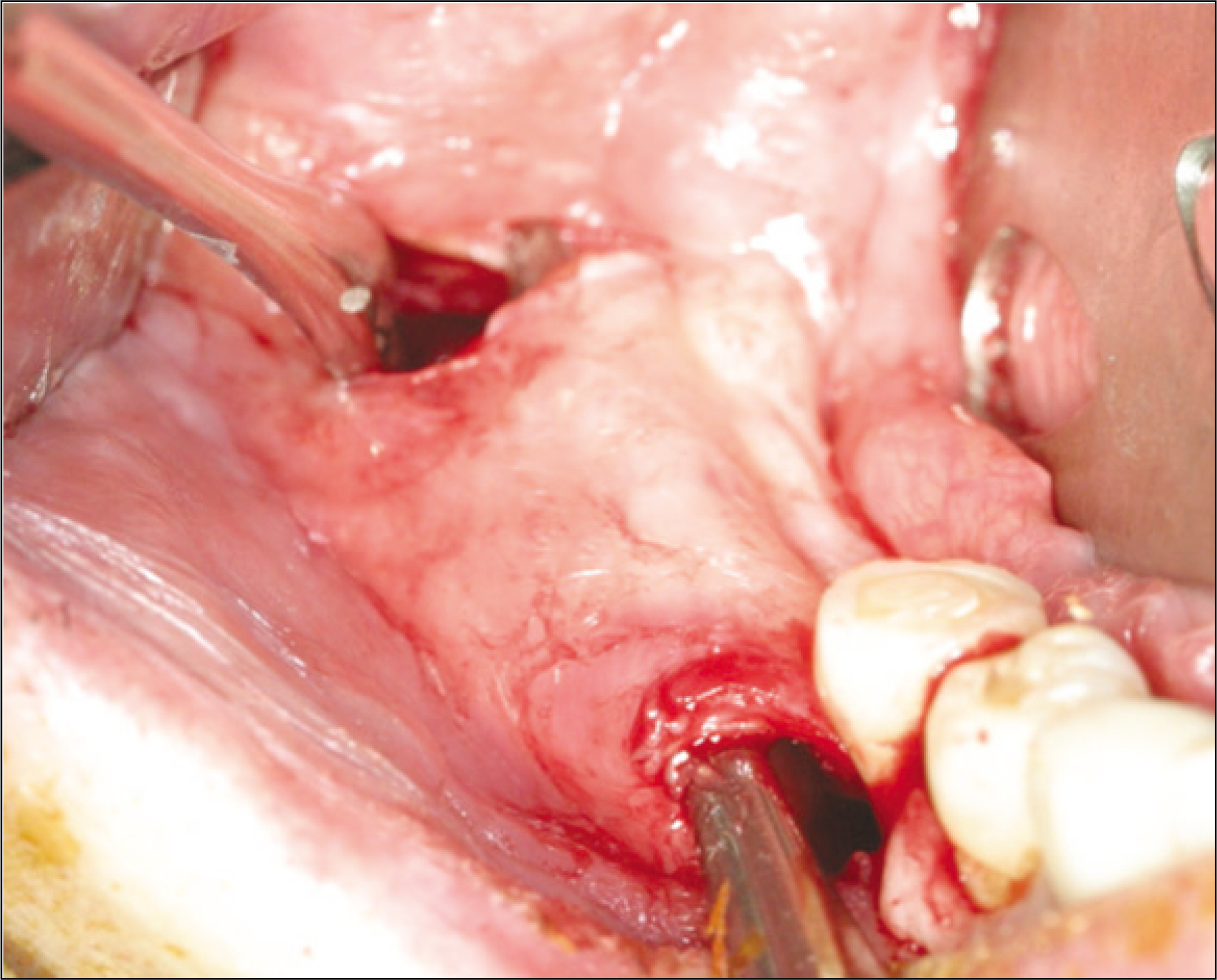
Fig. 6. Dissection and formation of subperiosteal pocket using sharp periosteal elevator.
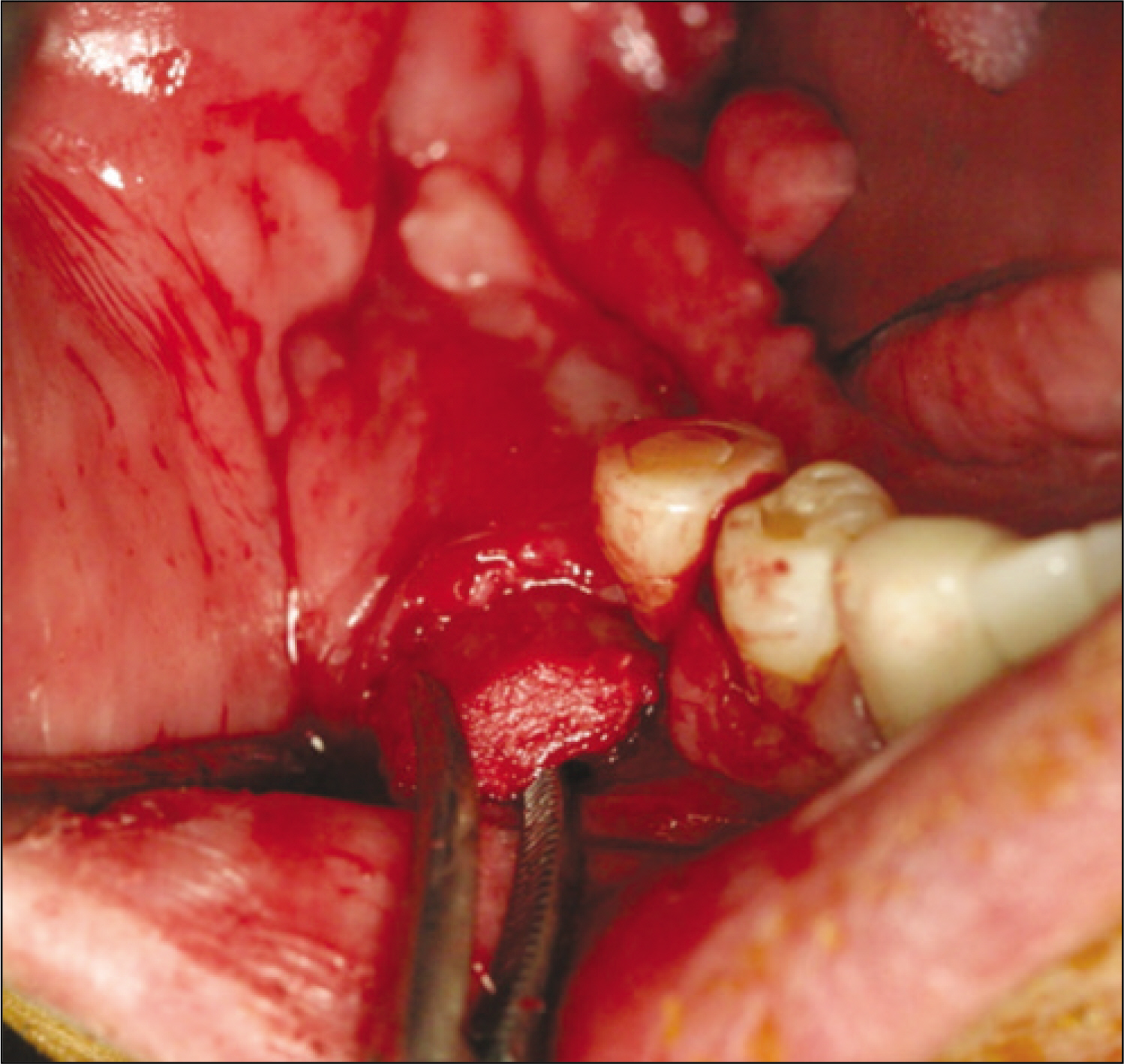
Fig. 7. Iliac corticocancellous block bone graft being inserted under the elevated subperiosteal pocket. Before insertion of the block, periosteal releasing incision was made with iris scissors. After insertion, the space between the recipient site and block was filled with bone chips mixed with FDBA (orthoblast II). (FDBA: freeze-dried bone allograft)

Fig. 8. Fixation of block bone with microscrew.

Fig. 9. Immediate postoperative view of the grafted alveolar ridge.
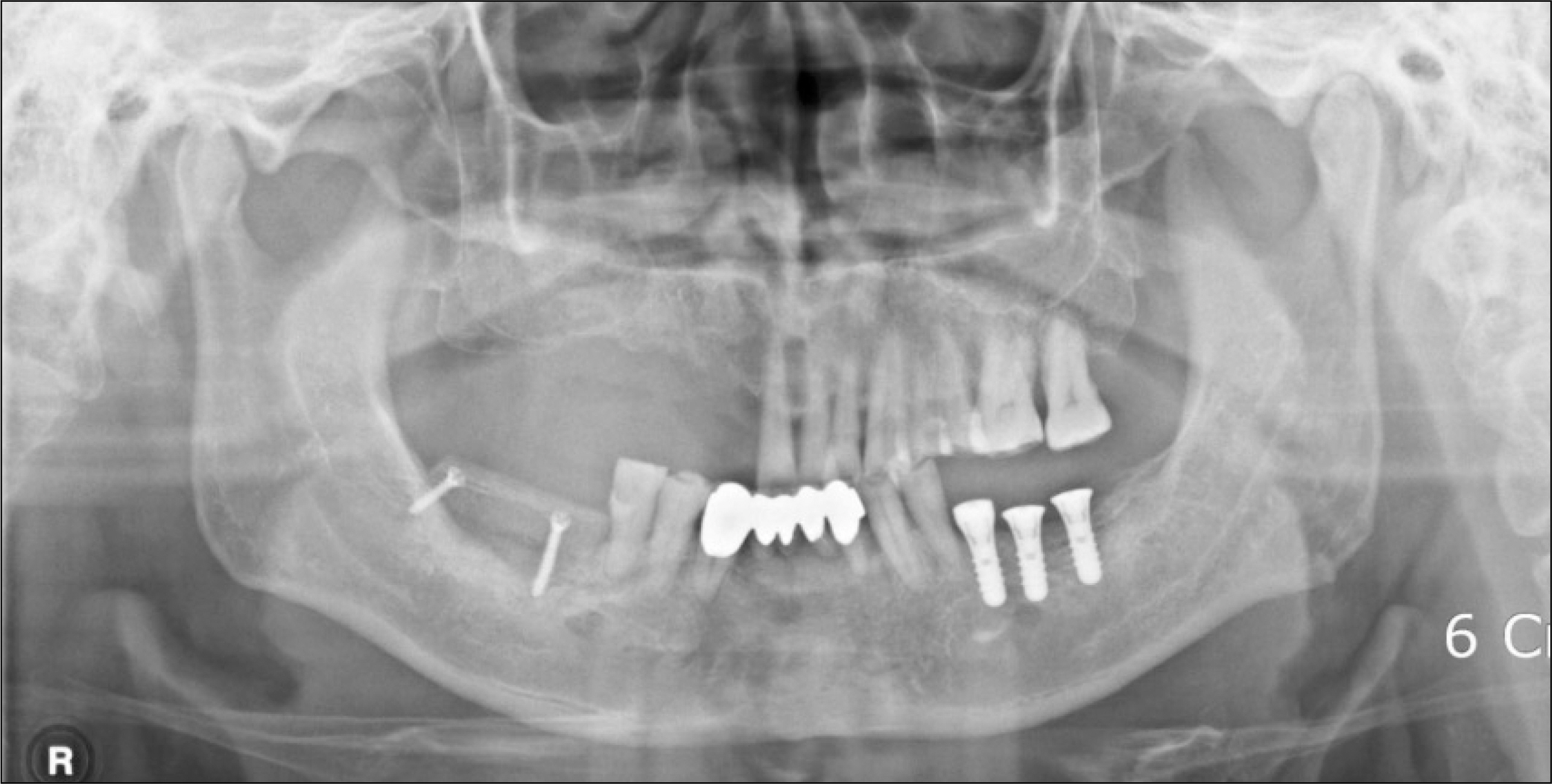
Fig. 10. Postoperative panoramic view showing grafted area of right posterior mandibular ridge.

Fig. 11. Postoperative conebeam computerized tomography (CBCT) scan after 4 months of healing of the graft showing augmented alveolar ridge on right posterior mandible.

Fig. 12. Two Implants were placed with more than 35 NCm torque on grafted sites with trans-gingival type fixture.

Fig. 13. The final prosthesis fabricated after 5 months of healing period of the implants in the graft.
Reference
-
References
1. Rocchietta I, Fontana F, Simion M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: a systematic review. J Clin Periodontol. 2008; 35(8 Suppl):203–15.
Article2. Felice P, Marchetti C, Piattelli A, Pellegrino G, Checchi V, Worthington H, et al. Vertical ridge augmentation of the atrophic posterior mandible with interpositional block grafts: bone from the iliac crest versus bovine anorganic bone. Eur J Oral Implantol. 2008; 1:183–98.3. Cordaro L, Amade ′DS, Cordaro M. Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement. Clin Oral Implants Res. 2002; 13:103–11.
Article4. Chiapasco M, Zaniboni M, Rimondini L. Autogenous onlay bone grafts vs. alveolar distraction osteogenesis for the correction of vertically deficient edentulous ridges: a 2–4-year prospective study on humans. Clin Oral Implants Res. 2007; 18:432–40.
Article5. Mecall RA, Rosenfield AL. The influence of residual ridge resorption patterns on implant fixture placement and tooth position. Part I. Int J Periodontics Restorative Dent. 1991; 11:8–23.6. Simion M, Trisi P, Piattelli A. Vertical ridge augmentation using a membrane technique associated with osseointegrated implants. Int J Periodontics Restorative Dent. 1994; 14:496–511.7. Rosenquist B. Implant placement in combination with nerve transpositioning: experiences with the first 100 cases. Int J Oral Maxillofac Implants. 1994; 9:522–31.
Article8. das Neves FD, Fones D, Bernardes SR, do Prado CJ, Neto AJ. Short implants – an analysis of longitudinal studies. Int J Oral Maxillofac Implants. 2006; 21:86–93.9. Esposito M, Grusovin MG, Kwan S, Worthington HV, Coulthard P. Interventions for replacing missing teeth: bone augmentation techniques for dental implant treatment. Cochrane Database Syst Rev. 2008; (3):CD003607. Review. Update in: Cochrane Database Syst Rev 2009;(4): CD003607.
Article10. McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992; 89:1–8. discussion 9–10.
Article11. Keller EE, Tolman DE, Eckert S. Surgical-prosthodontic reconstruction of advanced maxillary bone compromise with autogenous onlay block bone grafts and osseointegrated endosseous implants: a 12 year study of 32 consecutive patients. Int J Oral Maxillofac Implants. 1999; 14:197–209.12. Nystrom E, Ahlqvist J, Legrell PE, Kahnberg KE. Bone graft remodeling and implant success rate in the treatment of the severely resorbed maxilla: A 5 year longitudinal study. Int J Oral Maxillofac Surg. 2002; 31:158–64.13. Kent JN, Quinn JH, Zide MF, Guerra LR, Boyne PJ. Alveolar ridge augmentation using nonresorbable hydroxylapatite with or without autogenous cancellous bone. J Oral MaxilloFac Surg. 1983; 41:629–42.
Article14. Block MS, Degen M. Horizontal ridge augmentation using human mineralized particulate bone: preliminary results. J Oral Maxillofac Surg. 2004; 62(9 Suppl 2):67–72.
Article15. Hasson O. Augmentation of deficient lateral alveolar ridge using the subperiosteal tunneling dissection approach. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:e14–9.
Article16. Kfir E, Kfir V, Eliav E, Kaluski E. Minimally invasive guided bone regeneration. J Oral Implantol. 2007; 33:205–10.
Article17. Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988; 17:232–6.
Article18. Yerit KC, Posch M, Hainich S, Turhani D, Klug C, Wanschitz F, et al. Long-term implant survival in the grafted maxilla: results of a 12-year retrospective study. Clin Oral Implants Res. 2004; 15:693–9.
Article19. Reinert S, Konig S, Bremerich A, Eufinger H, Krimmel M. Stability of bone grafting and placement of implants in the severely atrophic maxilla. Br J Oral Maxillofac Surg. 2003; 41:249–55.
Article20. Verhoeven JW, Cune MS, Terlou M, Zoon MA, de Putter C. The combined use of endosteal implants and iliac crest onlay grafts in the severely atrophic mandible: a longitudinal study. Int J Oral Maxillofac Surg. 1997; 26:351–7.
Article21. Maiorana C, Beretta M, Salina S, Santoro F. Reduction of autogenous bone graft resorption by means of BioOss coverage: a prospective study. Int J Periodontics Restorative Dent. 2005; 25:19–25.22. Levin L, Herzberg R, Dolev E, Schwartz-Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. Int J Oral Maxillofac Implants. 2004; 19:369–73.
Article23. Rothstein SS, Paris DA, Zacek MP. Use of hydroxylapatite for the augmentation of deficient alveolar ridges. J Oral Maxillofac Surg. 1984; 42:224–30.
Article24. Khoury F. Augmentation osseuse et chirugie implantaire. Implant. 1999; 5:221–37.25. Ponte A, Khoury F. The tunnel technique in bone grafting procedures: a clinical study[abstract]. Int J Oral Maxillofac Implants. 2004; 19:766.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lateral alveolar ridge augmentation procedure using subperiosteal tunneling technique: a pilot study
- Minimal invasive horizontal ridge augmentation using subperiosteal tunneling technique
- Dental implant treatment with iliac bone graft via two-stage approach for avulsed alveolar bone defects; case report
- Implant Placement Using Alveolar Ridge Split in Atrophic Maxillary Alveolar Bone
- Ridge Augmentation Using Block Type of Autogenous Tooth Bone Graft Material in Severe Alveolar Bone Resorption of Single Tooth: Case Report
