Spinopelvic Reconstruction with Femoral Allograft and Vertical Rectus Abdominis Myocutaneous Flap after Total Sacrectomy in Recurrent Sacral Chordoma: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. bschang@snu.ac.kr
- KMID: 2328005
- DOI: http://doi.org/10.4184/jkss.2016.23.2.114
Abstract
- STUDY DESIGN: Case report.
OBJECTIVES
To report a case of recurrent sacral chordoma treated with total sacrectomy and spinopelvic reconstruction. SUMMARY OF LITERATURE REVIEW: Sacral chordoma is a musculoskeletal tumor reported to have a low incidence. Surgical treatment is considered difficult due to the complicated sacropelvic structure, so the prognosis for patients with sacral chordoma has been considered poor.
MATERIALS AND METHODS
We report a surgical technique and outcomes from spinopelvic reconstruction with femoral allograft and vertical rectus abdominis myocutaneous flap after total sacrectomy.
RESULTS
We report no tumor recurrence at 43 months postoperatively.
CONCLUSIONS
Spinopelvic reconstruction with thorough surgical planning after total sacrectomy was found to be a safe and effective treatment method.
MeSH Terms
Figure
-
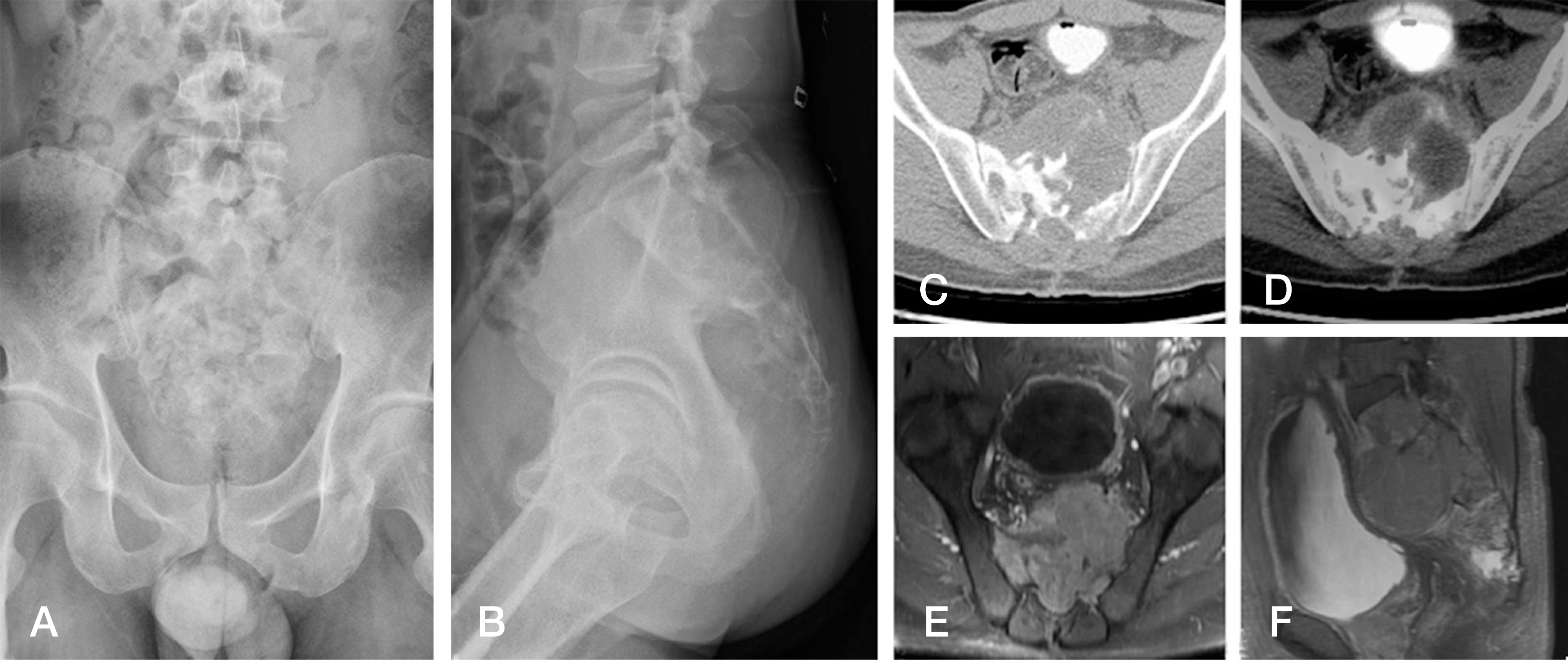
Fig. 1. Pelvic anteroposterior (A) and lateral radiographs (B) show a soft tissue mass in the presacral area with sacral destruction. The axial CT (C) and PET/CT (D) images show a destructive soft tissue mass with the rectum and bladder compressed at the S2 level. Gadolinium-enhanced fat-suppressed T1-weighted axial (E) and sagittal (F) MR images also show a large lobulating soft tissue mass destructing the sacrum.

Fig. 2. (A) An intraoperative photo shows harvesting of the vertical rectus abdominis myocutaneous flap. (B) An intraabdominal photo shows the ligated internal iliac artery (arrow). (C) A posterior incision bypassed the scar of the previous operation to eliminate the tumor. (D) The resected tumor mass with contaminated skin after total sacrectomy. (E) A femoral bone allograft between the iliac bone and L5 was fixed by a half-threaded cortical screw and pedicle, while an iliac screw and rod system was fixed for stabilization from L3 to the iliac bone. (F, G) Soft tissue reconstruction with a vertical rectus abdominis myocutaneous flap from the intraabdominal space was performed by a plastic surgeon. The pelvis anteroposterior (H) and lateral (I) radiographs show a total sacrectomy with spinopelvic reconstruction with a femoral allobone graft.
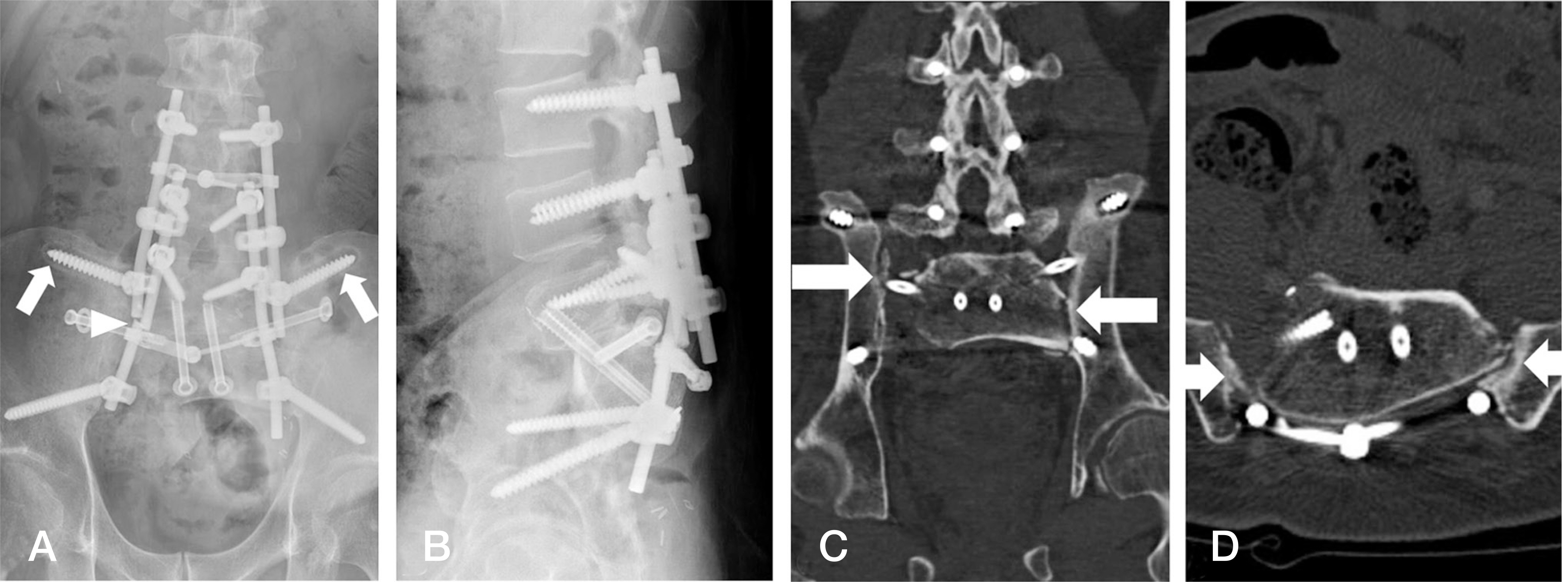
Fig. 3. The pelvis anteroposterior (A) and lateral (B) radiographs show loosening of the iliac screw (arrow) and rod breakage (arrowhead) at 31 months postoperatively. Axial (C) and sagittal (D) CT images show nonunion between the femoral allograft and both ilia (arrow).
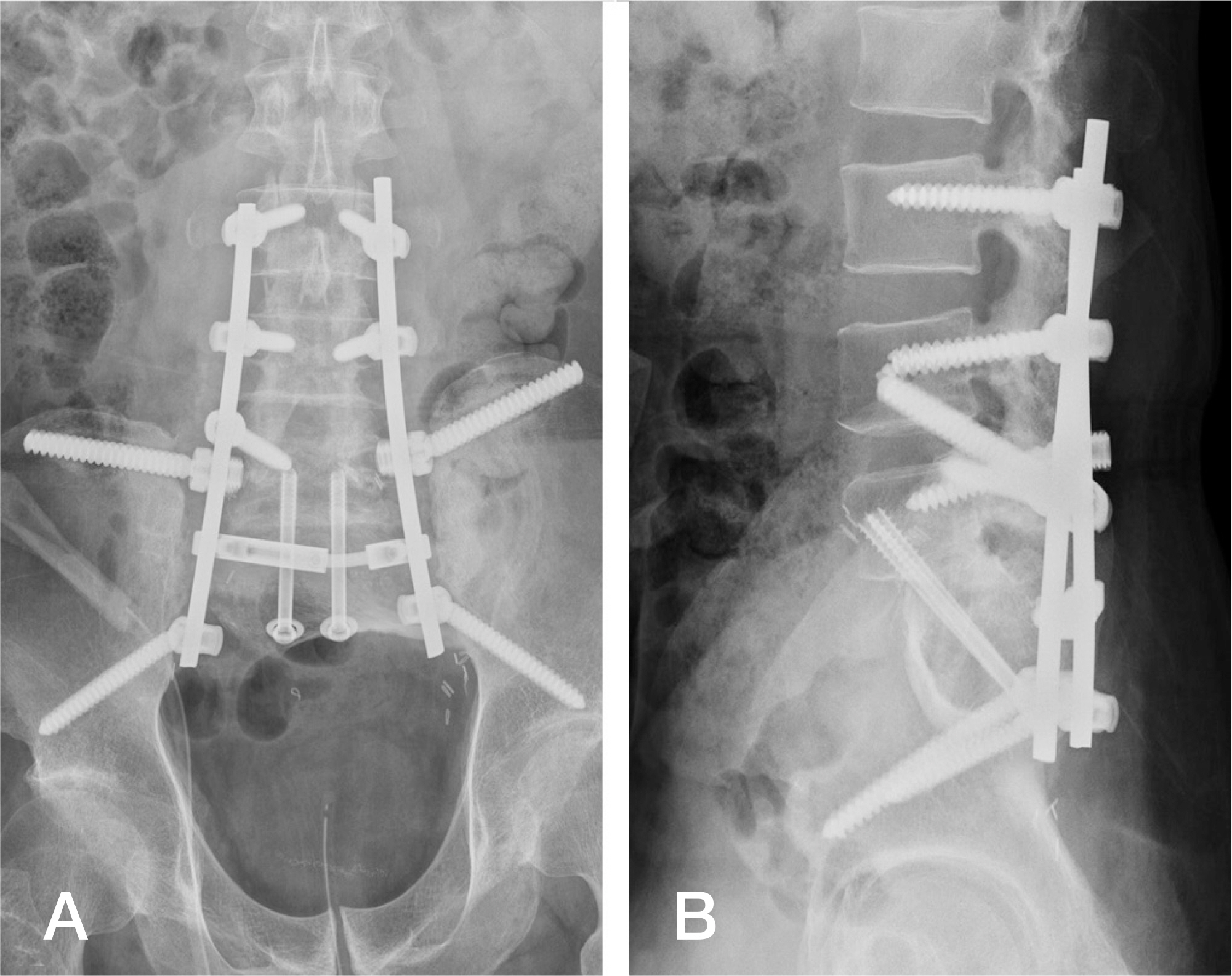
Fig. 4. After the second operation, the pelvics anteroposterior (A) and lateral (B) radiographs show the new iliac screw and rod with a fresh frozen allobone chip graft at the previous graft-ilium junction.

Fig. 5. The pelvis anteroposterior (A) and lateral (B) radiographs show well-maintained fixation and graft material.
Reference
-
1. Bederman SS, Shah KN, Hassan JM, et al. Surgical techniques for spinopelvic reconstruction following total sacrectomy: a systematic review. Eur Spine J. 2014; 23:305–19.
Article2. Todd LTJ, Yaszemski MJ, Currier BL, et al. Bowel and bladder function after major sacral resection. Clin Orthop Relat Res. 2002; 397:36–9.
Article3. Zhang HY, Thongtrangan I, Balabhadra RS, et al. Surgical techniques for total sacrectomy and spinopelvic reconstruction. Neurosurg Focus. 2003; 15:E5.
Article4. Bohinski RJ, Mendel E, Rhines LD. Novel use of a thread-wire saw for high sacral amputation. Technical note and description of operative technique. J Neurosurg Spine. 2005; 3:71–8.5. Shikata J, Yamamuro T, Kotoura Y, et al. Total sacrectomy and reconstruction for primary tumors. Report of two cases. J Bone Joint Surg Am. 1988; 70:122–5.
Article6. Blatter G, Halter Ward EG, Ruflin G, et al. The problem of stabilization after sacrectomy. Arch Orthop Trauma Surg. 1994; 114:40–2.
Article7. Wuisman P, Lieshout O, van Dijk M, et al. Reconstruction after total en bloc sacrectomy for osteosarcoma using a custom-made prosthesis: a technical note. Spine (Phila Pa 1976). 2001; 26:431–9.8. Gokaslan ZL, Romsdahl MM, Kroll SS, et al. Total sacrectomy and Galveston L-rod reconstruction for malignant neoplasms. Technical note. J Neurosurg. 1997; 87:781–7.9. Touny A, Othman H, Maamoon S, et al. Perineal reconstruction using pedicled vertical rectus abdominis myocutaneous flap (VRAM). J Surg Oncol. 2014; 110:752–7.
Article10. Guo Y, Palmer JL, Shen L, et al. Bowel and bladder con-tinence, wound healing, and functional outcomes in patients who underwent sacrectomy. J Neurosurg Spine. 2005; 3:106–10.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Breast Reconstruction with Free Transverse Rectus Abdominis Myocutaneous Flap Complicated by Deep Vein Thrombosis-associated Pulmonary Thrombo-embolism
- Rectus Abdominis Free Flap Reconstruction for Orbital-Maxillary Defect in Advanced Maxillary Sinus Cancer
- Vertical Rectus Abdominis Myocutaneous-Pedicled Island Flap for Covering Defect of the Suprapubic Area: A Case Report
- The Rectus Abdominis Myocutaneous Flap for the Immediate Reconstruction of Partial Vaginal Defects Following the Extended Abdominoperineal Resection of Recurrent Rectal Cancer
- Reconstruction of Midfacial Defect Using Various Free Flap
