Infect Chemother.
2016 Jun;48(2):91-98. 10.3947/ic.2016.48.2.91.
Anaerobic Bacteremia: Impact of Inappropriate Therapy on Mortality
- Affiliations
-
- 1Department of Laboratory Medicine and Research Institute of Bacterial Resistance, Yonsei University College of Medicine, Seoul, Korea. leekcp@yuhs.ac
- 2Department of Laboratory Medicine, Hanyang University College of Medicine, Seoul, Korea.
- 3Department of Laboratory Medicine, National Health Insurance Corporation, Ilsan Hospital, Goyang, Korea.
- 4Department of Internal Medicine and AIDS Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2327976
- DOI: http://doi.org/10.3947/ic.2016.48.2.91
Abstract
- BACKGROUND
Investigation on incidence and mortality of anaerobic bacteremia (AB) is clinically relevant in spite of its infrequent occurrence and not often explored, which report varies according to period and institutions. Therefore, it is necessary to analyze the incidence and risk factors related to mortality and assess clinical outcomes of AB in current aspect.
MATERIALS AND METHODS
Characteristics of AB patients and anaerobic bacteria from blood culture at a university hospital in 2012 were reviewed retrospectively. The correlation between risk factors and 28-day patient mortality was analyzed.
RESULTS
A total of 70 non-duplicated anaerobic bacteria were isolated from blood of 70 bacteremia patients in 2012. The history of cardiovascular disease as host's risk factor was statistically significant (P = 0.0344) in univariate and multivariate analysis. Although the inappropriate therapy was not statistically significant in univariate and multivariate analysis, the survival rate of bacteremia was significantly worse in patients who had inappropriate therapy compared with those underwent appropriate therapy (hazard ratio, 5.4; 95% confidence interval, 1.7-6.9; P = 0.004). The most frequently isolated organism was Bacteroides fragilis (32 isolates, 46%), followed by Bacteroides thetaiotaomicron (10, 14%), and non-perfringens Clostridium (7, 10%).
CONCLUSION
The incidence of AB in 2012 was 2.3% (number of AB patients per 100 positive blood culture patients) and the mortality rate in patients with clinically significant AB was 21.4%. In addition, AB was frequently noted in patients having malignancy and the survival rate of AB was significantly worse in patients who received inappropriate therapy compared with those underwent appropriate therapy.
MeSH Terms
Figure
-
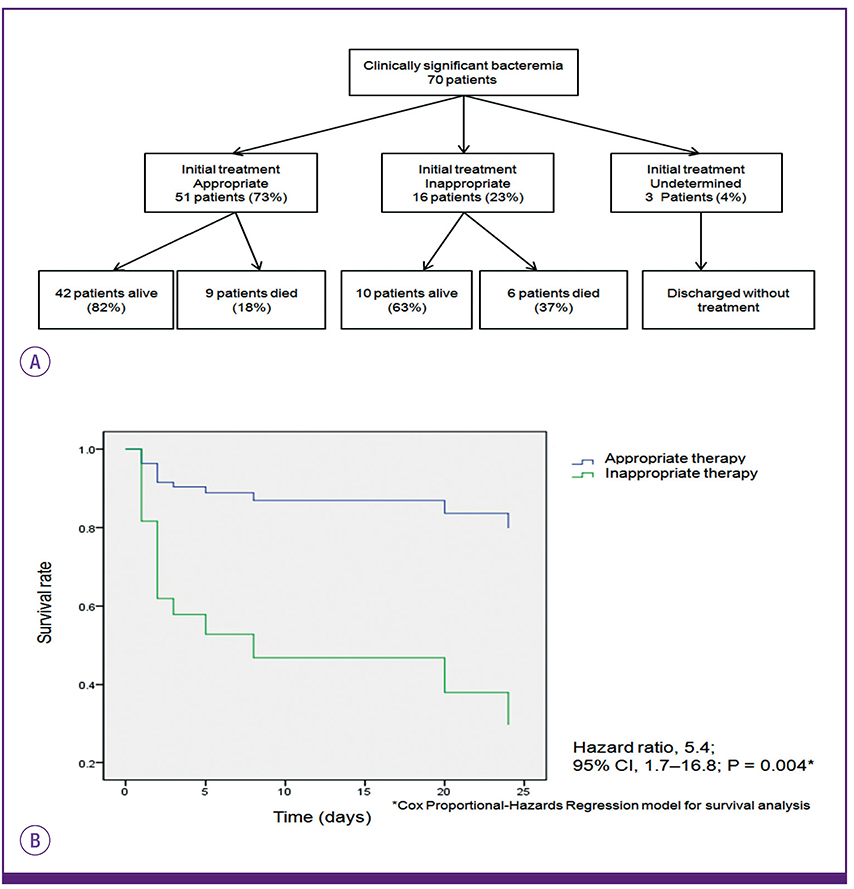
Figure 1 Clinical outcome and survival rate of 70 patients with anaerobic bacteremia according to appropriateness of treatment(A, B).
Cited by 2 articles
-
The Importance of the Early and Appropriate Treatment of Anaerobic Bacteremia Patients
Young Ah Kim
Infect Chemother. 2016;48(2):143-144. doi: 10.3947/ic.2016.48.2.143.Clinical and Therapeutic Implications of Aeromonas Bacteremia: 14 Years Nation-Wide Experiences in Korea
Ji Young Rhee, Dong Sik Jung, Kyong Ran Peck
Infect Chemother. 2016;48(4):274-284. doi: 10.3947/ic.2016.48.4.274.
Reference
-
1. Washington JA 2nd. Comparison of two commercially available media for detection of bacteremia. Appl Microbiol. 1971; 22:604–607.
Article2. Arzese A, Trevisan R, Menozzi MG. Anaerobe-induced bacteremia in Italy: a nationwide survey. The Italian Anaerobe Study Group. Clin Infect Dis. 1995; 20:Suppl 2. S230–S232.3. Peraino VA, Cross SA, Goldstein EJ. Incidence and clinical significance of anaerobic bacteremia in a community hospital. Clin Infect Dis. 1993; 16:Suppl 4. S288–S291.
Article4. Vazquez F, Mendez FJ, Perez F, Mendoza MC. Anaerobic bacteremia in a general hospital: retrospective five-year analysis. Rev Infect Dis. 1987; 9:1038–1043.
Article5. Wilson JR, Limaye AP. Risk factors for mortality in patients with anaerobic bacteremia. Eur J Clin Microbiol Infect Dis. 2004; 23:310–316.
Article6. Salonen JH, Eerola E, Meurman O. Clinical significance and outcome of anaerobic bacteremia. Clin Infect Dis. 1998; 26:1413–1417.
Article7. Cheng CW, Lin HS, Ye JJ, Yang CC, Chiang PC, Wu TS, Lee MH. Clinical significance of and outcomes for Bacteroides fragilis bacteremia. J Microbiol Immunol Infect. 2009; 42:243–250.8. Summanen P, Baron EJ, Citron DM, Strong CA, Wexler HM, Finegold SM. Wadsworth anaerobic bacteriology manual. 5th ed. Belmont, CA: Star Publishing Co.;1993.9. Clinical and Laboratory Standards Institute (CLSI). Methods for antimicrobial susceptibility testing of anaerobic bacteria : approved standard. 8th ed. Wayne, PA: CLSI;2012.10. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G. SCCM/ESICM/ACCP/ATS/SIS. 2001 SCCM/ESICM/ACCP/ATS/SIS International sepsis definitions conference. Crit Care Med. 2003; 31:1250–1256.
Article11. Lenz R, Leal JR, Church DL, Gregson DB, Ross T, Laupland KB. The distinct category of healthcare associated bloodstream infections. BMC Infect Dis. 2012; 12:85.
Article12. Weinstein MP, Towns ML, Quartey SM, Mirrett S, Reimer LG, Parmigiani G, Reller LB. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997; 24:584–602.
Article13. Brook I. Treatment of anaerobic infection. Expert Rev Anti Infect Ther. 2007; 5:991–1006.
Article14. Nguyen MH, Yu VL, Morris AJ, McDermott L, Wagener MW, Harrell L, Snydman DR. Antimicrobial resistance and clinical outcome of Bacteroides bacteremia: findings of a multicenter prospective observational trial. Clin Infect Dis. 2000; 30:870–876.
Article15. Lassmann B, Gustafson DR, Wood CM, Rosenblatt JE. Reemergence of anaerobic bacteremia. Clin Infect Dis. 2007; 44:895–900.
Article16. Kim HO, Kang CG, Chong Y, Lee SY. Organisms isolated from blood at the Yonsei medical center, 1974-1983. Korean J Infect Dis. 1985; 17:15–32.17. Koh EM, Lee SG, Kim CK, Kim M, Yong D, Lee K, Kim JM, Kim DS, Chong Y. Microorganisms isolated from blood cultures and their antimicrobial susceptibility patterns at a university hospital during 1994-2003. Korean J Lab Med. 2007; 27:265–275.
Article18. Park Y, Lee Y, Kim M, Choi JY, Yong D, Jeong SH, Kim JM, Lee K, Chong Y. Recent trends of anaerobic bacteria isolated from clinical specimens and clinical characteristics of anaerobic bacteremia. Infect Chemother. 2009; 41:216–223.
Article19. Do SR. Changing trends in Korean patients' use of health facilities. Accessed 12 February 2016. Available at: https://www.kihasa.re.kr/web/publication/periodical/issue_view.do?menuId=50&tid=38&bid=21&searchForm=Y&keyField=myear&search-Stat=2009&key=&aid=8&ano=1.20. Yang CC, Hsu PC, Chang HJ, Cheng CW, Lee MH. Clinical significance and outcomes of Clostridium perfringens bacteremia--a 10-year experience at a tertiary care hospital. Int J Infect Dis. 2013; 17:e955–e960.21. Kornowski R, Schwartz D, Averbuch M, Levo Y, Berger S, Giladi M. Anaerobic bacteremia: a retrospective four-year analysis in general medicine and cancer-patients. Infection. 1993; 21:241–244.
Article22. Robert R, Deraignac A, Le Moal G, Ragot S, Grollier G. Prognostic factors and impact of antibiotherapy in 117 cases of anaerobic bacteraemia. Eur J Clin Microbiol Infect Dis. 2008; 27:671–678.
Article23. Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000; 31:Suppl 4. S131–S138.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Impact of Inappropriate Empirical Antibiotic on Outcomes in Community-acquired Third Generation Cephalosporin Resistant Enterobacterales Bacteremia
- Recent Trends of Anaerobic Bacteria Isolated from Clinical Specimens and Clinical Characteristics of Anaerobic Bacteremia
- Eleven-Year Experience of Clostridial Bacteremia at a Tertiary Care Hospital in South Korea
- Risk Factors for Mortality in Patients with Carbapenem-Resistant Acinetobacter baumannii Bacteremia: Impact of Appropriate Antimicrobial Therapy
- The Importance of the Early and Appropriate Treatment of Anaerobic Bacteremia Patients
