J Korean Soc Spine Surg.
2006 Dec;13(4):234-239.
Mono-segment Cervical Spondylotic Myelopathy
- Affiliations
-
- 1Department of Orthopedic Surgery, SUN Hospital, Daejeon, Korea. chspine@korea.com
Abstract
-
STUDY DESIGN: A retrospective follow-up study comparing soft disc cervical myelopathy (Group A) and spondylotic bar cervical myelopathy (Group B).
OBJECTIVES
To analyze different factors by comparing preoperative radiological and clinical data of Group A with that of Group B. SUMMARY AND LITERATURE REVIEW: The different causes of cervcal myelopathy resulted in different symptoms and prognoses. MATERIALS AND METHOD: A clinical and radiological analysis of the data in 31 patients who underwent an anterior cervical decompression and fusion was performed to assess the different factors between two groups. The patients were classified into two groups; 20 in Group A and 11 in Group B. Comparisons between the two groups were made in regard to the physical findings, radiological and clinical evaluation.
RESULTS
The duration of myelopathy was 3 months in Group A and 8.7months in Group B. Of all cases, 5 cases (25.0%) in group A and 4 cases (36.4%) in group B had myelopathy associated with radiculopathy. Of the 20 cases in group A with myelopathy, 7 cases had a median compression and 13 cases had a paramedian compression on MRI. Of the 11 cases in group B with meylopathy, 9 cases had a median compression and 2 cases had a paramedian compression on MRI. The follow-up MRI of the 14 cases (73.7%) in group A and 2 cases (20.0%) in group B showed spontaneous regression of the T2 WI high signal intensity.
CONCLUSION
In degenerative disc disease, the different causes of cervcal myelopathy result in different symptoms and prognoses. However, the treatment of choice in both groups is a one level anterior decompression and fusion.
MeSH Terms
Figure
-
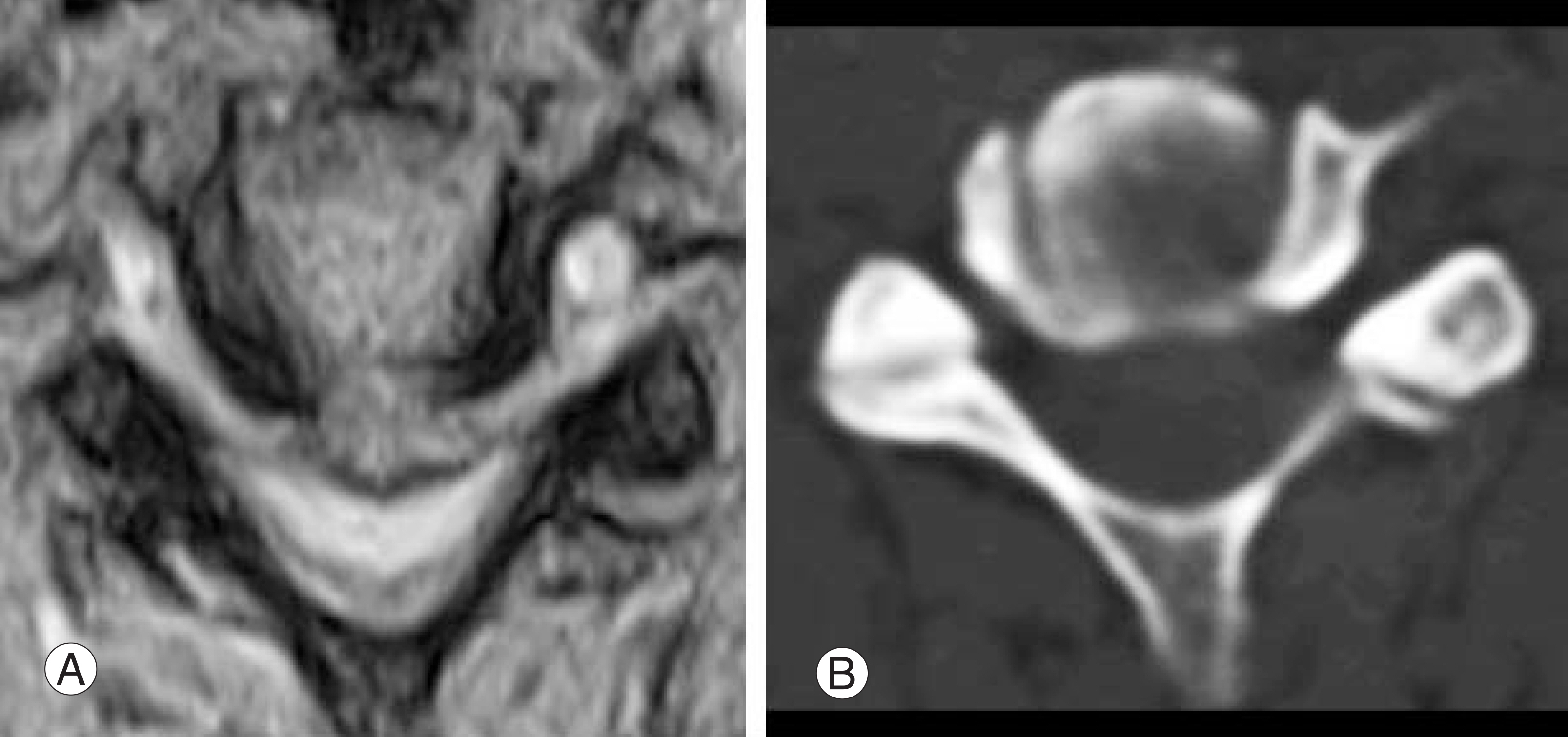
Fig. 1. cervical myelopathy due to soft disc on axial view of T2 WI MRI and CT.
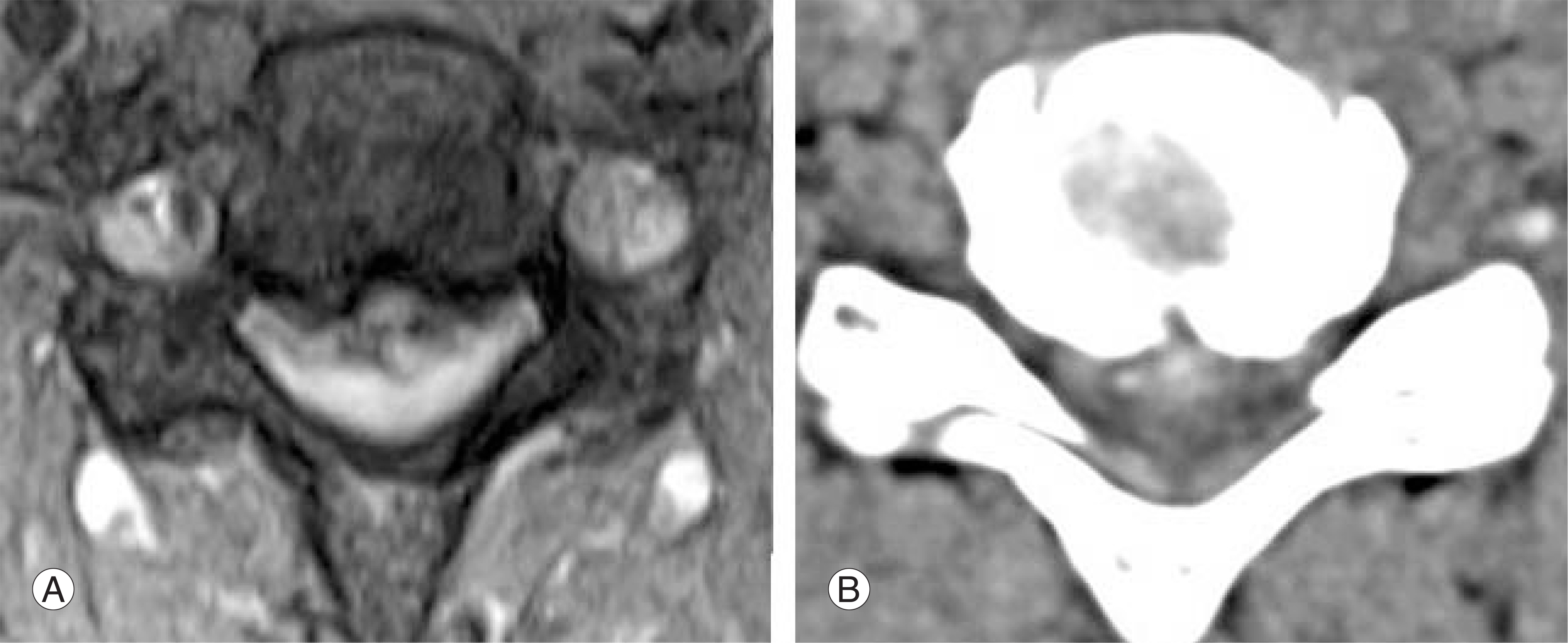
Fig. 2. cervical myelopathy due to spondylotic bar on axial view of T2 WI MRI and CT.

Fig. 3. cervical myelopathy due to soft disc on sagittal view of T2 WI preoperative and postoperative MRI.
Reference
-
1). Aldrich F. Posterolateral microdiscectomy for cervical monoradiculopathy caused by posterolateral soft cervical disc sequestration. J Neurosurg. 72:370–377. 1990.
Article2). Lestini WF, Wiesel SW. The pathogenesis of cervical spondylosis. Clin Orthop. 239:69–93. 1989.
Article3). Lunsford LD, Bissonette DJ, Jannetta PJ, Sheptak PE, Zorub DS. Anterior surgery for cervical disc disease: Part I. Treatment of lateral cervical disc herniation in 253 cases. J Neurosurg. 53:1–11. 1980.4). Mosdal C. Cervical ostochondrosis and disc herniation: Eighteen years use of Interbody fusion by Cloward's technique in 755 cases. Acta Neurochir. 70:207–225. 1984.5). Murphey F, Simmons JC, Brunson B. Surgical treatment of laterally ruptured cervical disc: Review of 648 cases, 1939 to 1972. J Neurosurg. 38:679–683. 1973.6). Bemgard M, Hynes RA, Blume HW, White III AA. Cervical spondylotic myelopathy. J Bone Joint Surg. 75-A:120–128. 1993.7). Shin Y, Shoichi K, Yushin I, Yasuhisa T. Courses of cervical disc herniation causing myelopathy or radiculopathy. Spine. 28:1171–1175. 2003.8). Hayashi K, Yabuki T, Kurokawa T, Seki H, Hogaki M, Minoura S. The anterior and the posterior longitudinal ligaments of the lower cervical spine. J Anat. 124:633–636. 1977.9). Sasaki T. Considerations on the nature of the ossification of posterior longitudinal ligamentum of the cervical spine (in Japanese). Saigaiigaku. 18:663–669. 1975.10). Sasaki T, Hosokawa M, Ukai S, et al. .:. Anatomy of the anterior and posterior longitudinal ligament on the cervical spine (in Japanese). Central Jpn J orthop Trauma. 19:893–895. 1976.11). Suzuki Y. An anatomical study on the anterior and posterior longitudinal ligament of the spinal column: especially on its fine structure and ossifying disease process (in Japanese). J Jpn J Orthop Assoc. 46:179–195. 1972.12). Parke WW. Correlative anatomy of cervical spondylotic myelopathy. Spine. 7:831–837. 1988.
Article13). Debois V, Herz R, Berghmans D, Hermans B, Herre-qodts P. Soft cervical disc herniation. Influence of cervical spinal canal measurements on development of neurologic symptoms. Spine. 24:1996–2002. 1999.14). Wada E, Yonenobu K, Suzuki S, Kanazawa A, Ochi T. Can intramedullary signal change on magnetic resonance predict surgical outcome in cervical spondylotic myelopathy? Spine. 24:455–461. 1999.15). Faiss JH, Schroth G, Grodd W, Koeing E, Will B, Thron A. Central spinal cord lesions in stenosis of the cervical canal. Neuroradiology. 32:117–123. 1990.
Article16). Iwasaki Y, Abe H, Isu T, Miyasaki K. CT myelography with intramedullary enhancement in cervical spondylosis. J Neurosurg. 63:363–366. 1985.
Article17). Scoville WB, Dohrmann GJ, Corkill G. Late results of cervical disc surgery. J Neurosurg. 45:203–210. 1976.
Article18). Francois A. Posterolateral microdisectomy for cervical monoradiculopathy caused by posterolateral soft cervical disc sequestration. J Neurosurg. 72:370–377. 1990.19). Williams RW. Microcervical foraminotomy: a surgical alternative for intractable radicular pain. Spine. 8:708–716. 1983.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retraction: Sensitivity of Pyramidal Signs in Patients with Cervical Spondylotic Myelopathy
- Vertebral Body Sliding Osteotomy for Cervical Myelopathy With Rigid Kyphosis
- Surgical Treatment of Cervical Spondylotic Myelopathy
- Cervical spondylotic myelopathy and radiculopathy: a stepwise approach and comparative analysis of surgical outcomes: a narrative review of recent literature
- Value of Surgery and Nonsurgical Approaches for Cervical Spondylotic Myelopathy: WFNS Spine Committee Recommendations
