J Korean Soc Spine Surg.
2004 Dec;11(4):210-215.
Safe Approaching Angle and Distance in Percutaneous Endoscopic Discectomy
- Affiliations
-
- 1Department of Orthopedic Surgery, Gangneung Asan Hospital, College of Medicine, Ulsan University, Gangneung, Korea. eugene@gnah.co.kr
- 2Department of Radiology, Gangneung Asan Hospital, College of Medicine, Ulsan University, Gangneung, Korea.
Abstract
- STUDY DESIGN: A retrograde study, using Computerized Tomography (CT), to evaluate a safer approaching angle and distance for a percutaneous endoscopic discectomy.
OBJECTIVES
To measure the safest approaching angle and distance in a percutaneous endoscopic discectomy at each vertebra level in Koreans. LITERATURE REVIEW SUMMARY: Some authors have shown an approaching angle of between 25 to 30 degrees, but reports on Koreans patients are very rare.
MATERIALS AND METHODS
200 cases of abdomino-pelvic CT were investigated. The minimal angle of safe approach was composed of two lines, one horizontal line passing through the mid point in the posterior cortex of upper vertebra, with the other extending passed the mid point of posterior cortex in the upper vertebra to the dorsal margin of the retroperitoneal fat or peritoneum. The maximal distance for a safe approach was measured from the end of spinous process to the point where the extended former second line crosses the skin. The minimal angles and maximal distances for safe approaches in males and females, from the right and left sides, at each level of the intervertebral space and in groups according to the BMI were compared.
RESULTS
Females had a larger mean minimal angle for a safe approach (14.7 degrees) than that for males (9.6 degrees). However, no differences were observed between the right (12.0 degrees) and left sides (12.4 degrees). At each vertebral level, L2-3(16.4 degrees), L3-4(11.3 degrees) and L4-5(8.8 degrees), significant differences were observed. However, obesity had no influence on the different angles for a safe approach. The maximal distances for safe approaches were 12.9 and 12,6cm in males and female, 12.8 cm in for both of the right and left sides, and 11.8, 13.0 and 13.6cm in L2-3, L3-4 and L4-5, respectively. No differences were observed in any of the above group, but the more obese group had a longer distance.
CONCLUSIONS
Females and the upper level of the intervertebral space had larger minimal angles for a safe approach, but there were no differences in relation to gender, direction and obesity. All the maximal distances for safe approaches were the same in males, females, right and left, and at each level of the intervertebral space, but the more obese group had a longer distance. A safer zone for the approach in a percutaneous endoscopic lumbar discectomy can be taken, considering the gender, vertebra level and obesity.
Keyword
Figure
-
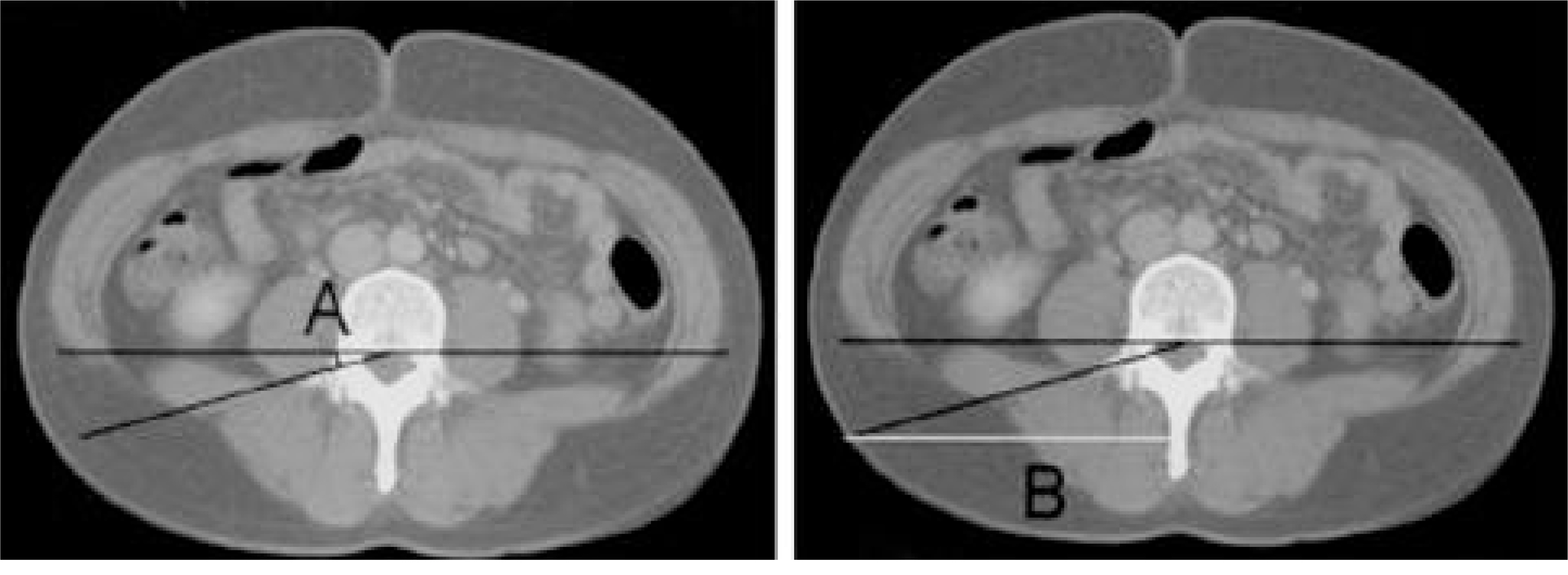
Fig. 1. 4th lumbar vertebral body in axial view of abodomino-pelvic CT. (A) shows minimal angle of safe approach (B) shows maximal distance of safe approach.
Reference
-
1). Kambin P. Arthroscopic microdiscectomy. Arthroscopy. 1992; 8:287–295.
Article2). Mathews HH. Transforaminal endoscopic microdiscectomy. Neurosurg Clin N Am. 1996; 7:59–63.
Article3). Kim JD. Micro endoscopic discectomy. J. Kor Spine Surg. 2000; 7:298–302.4). Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complication in 307 consecutive cases. Spine. 2002; 27(7):722–731.5). Hijikata S, Yamagishi M, Nakayama T, Oomori K. Percutaneous nuclectomy: A new treatment method for lumbar disc herniation. J. Tokyo Den-ryoku Hosp. 1975; 5:39–44.6). Hijikata S. Percutaneous nucleotomy: A new concept technique and 12 years experience. Clin. Orthop. 1988; 238:9–23.7). Kambin P, Gellman H. Percutaneous lateral discectomy of the lumbar spine: A preliminary report. Clin Orthop. 1983; 174:127–132.8). Kambin P, O’ brien E, Zhou L, et al. Art hroscop ic microdiscectomy and selective fragmentectomy. Clin Orthop. 1998; 347:150–167.9). Lew SM, Mehalic TF, Fagone KL. Transforaminal percutaneous endoscopic discectomy in the treatment of far-lateral and foraminal lumbar disc herniations. J Neurosurg Spine. 2001; 94:216–220.
Article10). Kambin P, Savitz MH. Arthroscopic microdiscectomy: An alternative to open disc surgery. Mt Sinai J Med. 2000; 67(4):283–287.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Endoscopic Discectomy for Lumbar Disc Herniation
- Entry Point and Approaching Angle of Working Cannula in Endoscopic Lumbar Disecectomy
- Pyogenic Spondylodiscitis after Percutaneous Endoscopic Lumbar Discectomy
- Percutaneous Endoscopic Interlaminar Discectomy for L5-S1 Disc Herniation: Axillary Approach and Preliminary Results
- Percutaneous Endoscopic Discectomy Compared to Microsurgical Discectomy: Preliminary Results
