J Korean Soc Spine Surg.
2002 Jun;9(2):115-120.
Significance of Chin-brow Vertical Angle in Correction of Kyphotic Deformity of Ankylosing Spondylitis Patients
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Kyung Hee University, Seoul, Korea. sks111@khmc.or.kr
- 2Department of Orthopaedic Surgery, Samsung Medical Center, Sungkyunkwan University, Seoul, Korea.
Abstract
-
STUDY DESIGN: Retrospective study of 34 ankylosing spondylitis patients with kyphotic deformity who performed correction osteotomy.
OBJECTIVES
To assess significance of chin-brow vertical angle for planning and evaluating correction of kyphotic deformity with ankylosis of cervical spine in ankylosing spondylitis patients. SUMMARY OF LITERATURE REVIEW: Accurate assessment and measurement of spinal kyphotic deformity is required when planning treatment and assessing its results. The most reliable measure of trunk deformity is the chin-brow vertical angle.
MATERIALS AND METHODS
Thirty-four ankylosing spondylitis patients with cervical ankylosis who had underwent pedicle subtraction extension osteotomy for correction of kyphotic deformity were studied. The patients consisted of 32 male and 2 female patients. Mean age was 35.7 years. Most common apex of kyphosis was T12 in 11 cases. The levels of osteotomy were L1 in 3 case, L2 in 4 cases, L3 in 17 cases, and L4 in 10 cases. Radiographic assessment for sagittal balance was performed by measuring thoracic kyphosis, lumbar lordosis, and distance between the vertical line on anterosuperior point of T1 and that of S1. Chin brow-vertical angle was measured on the preoperative and postoperative clinical photo of the patients. Clinical outcomes were assessed by questionnaire measuring changes in physical function, indoor activity, outdoor activity, psychosocial activity, pain, and patient 's satisfaction with the surgery.
RESULTS
Chin brow-vertical angle was 35.5 degrees preoperatively and 1.8 degrees postoperatively. Final follow-up radiograph showed an increase in lumbar lordosis from 5.5 to 43.2 degrees(an increase of 37.7 degrees) while thoracic kyphosis remain stable from 50.4 to 50.2 degrees. Sagittal imbalance significantly improved from 101.5 to12.7 mm. Decreased chin-brow vertical angle correlated negatively with correction angle while chin-brow vertical angle did not correlate with overall clinical outcome. However, the patients with chin brow vertical angle greater than 10 degrees or less than -10 degree had significantly low score concerning the item of horizontal gaze.
CONCLUSIONS
The ankylosing spondylitis patient with cervical ankylosis, who had chin-brow vertical angle ranging from -10 to 10 degrees, had better horizontal gaze. Based on the results of this study, measurement of chin-brow vertical angle was recom-mended for planning correction of kyphosis and accurate evaluation of treatment outcome.
MeSH Terms
Figure
-
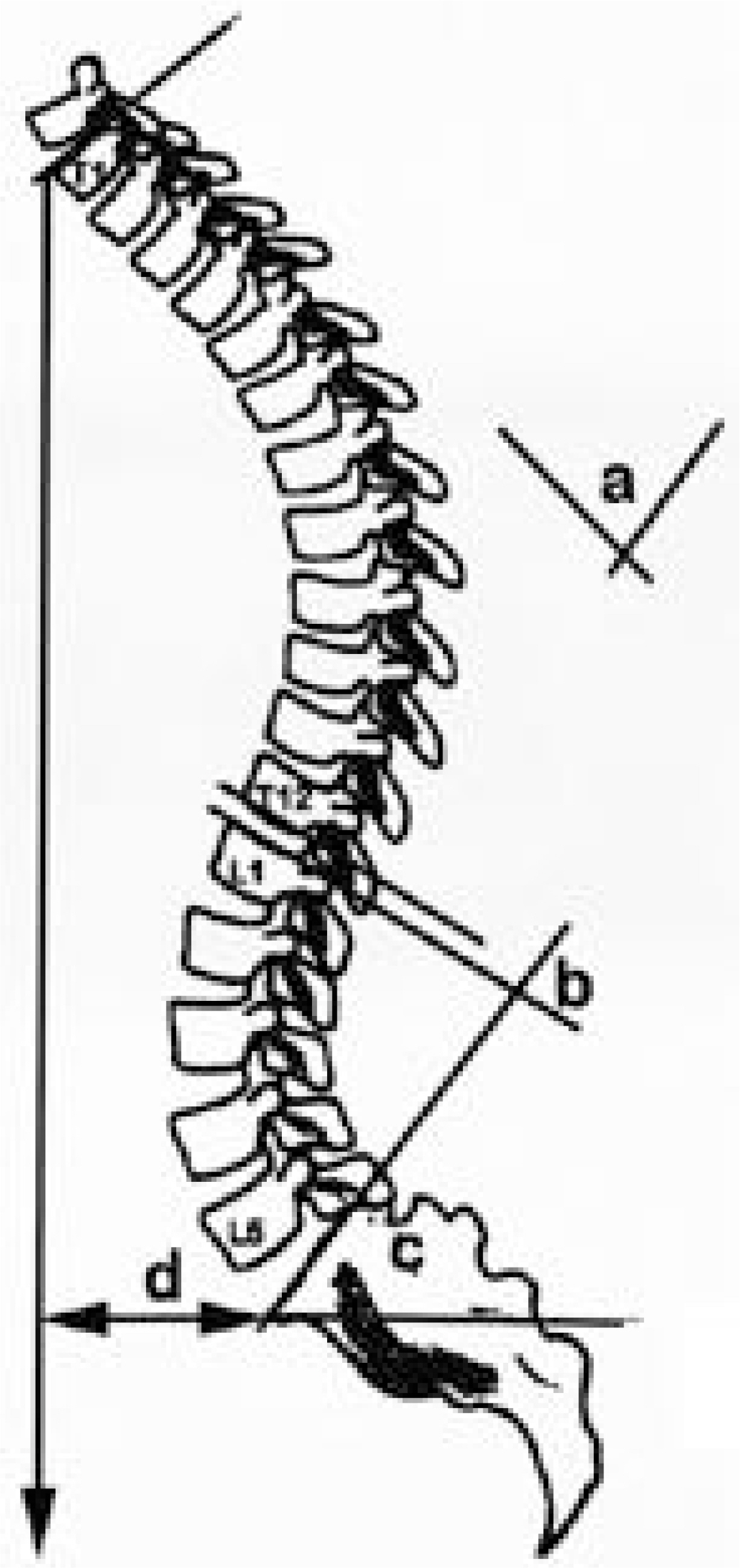
Fig. 1. The parameters for radiological measurements(a: thoracic kyphosis, b: lumbar lordosis, d: distance between the vertical line on anterosuperior point of T1 and that of S1).

Fig. 2. Clinical photo of a 45-year old patient. A. Preoperative chin brow vertical angle was 96 degrees and postoperative chin brow vertical angle was 17 degrees. B. Even though, chin brow vertical angle was undercorrected, he could get good horizontal gaze after surgery.
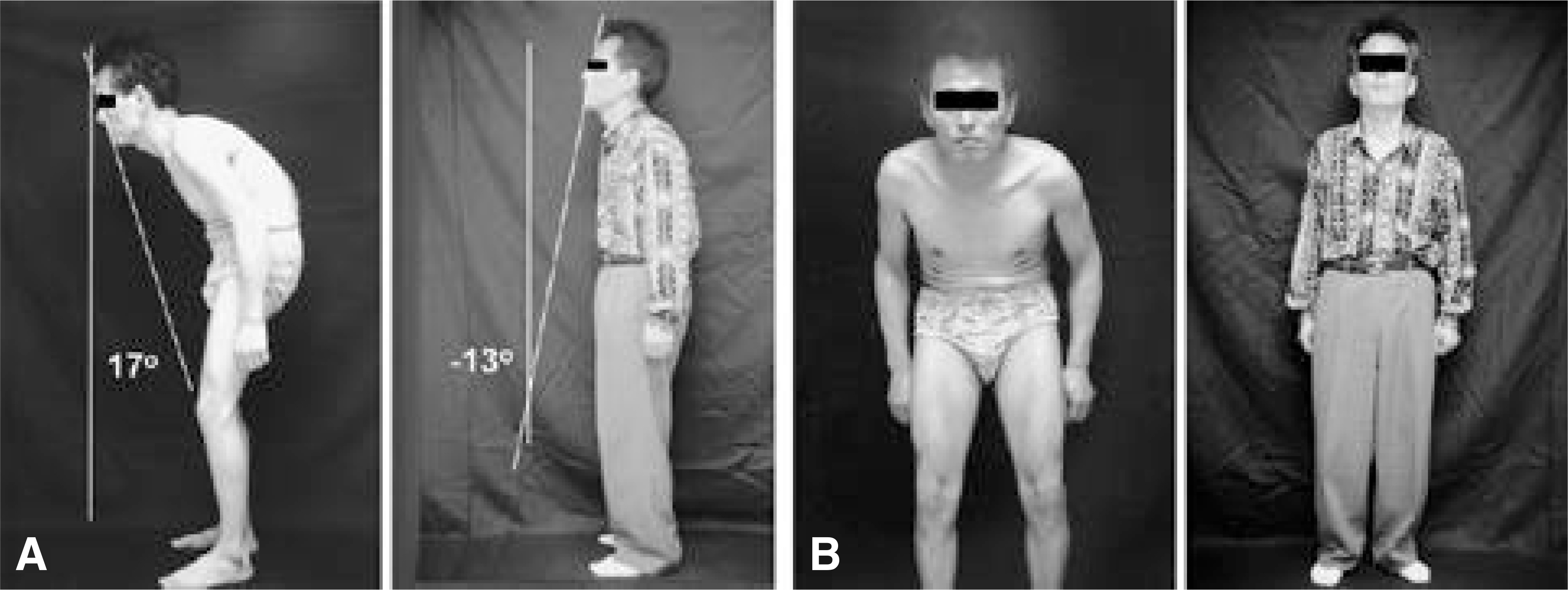
Fig. 3. Clinical photo of a 37-year old patient. A. Preoperative chin brow vertical angle was 17 degrees and postoperative chin brow vertical angle was -13 degrees. B. Chin brow vertical angle was overcorrected and he could not look straight forward after surgery.
Reference
-
1). Berven SH, Deviren V, Smith JA, Emami A, Hu SS, Bradford DS. Management of fixed sagittal plane deformity: Results of the transpedicular wedge resection osteotomy. Spine. 26(18):2036–2043. 2001.2). Bridwell KH, DeWald RL. The textbook of spinal surgery. 2nd ed.Philadelphia: Lippincott-Raven;p. 1133. 1997.3). Camargo FP, Cordeiro EN, Napoli MM. Corrective osteotomy of the spine in ankylosing spondylitis. Experience with 66 cases. Clin Orthop. 208:157–167. 1986.4). Chen IH, Chien JT, Yu TC. Transpedicular wedge osteotomy for correction of thoracolumbar kyphosis in ankylosing spondylitis: experience with 78 patients. Spine. 26(16):E354–360. 2001.5). Danisa OA, Turner D, Richardson WJ. Surg ical correction of lumbar kyphotic deformity: posteior reduction “eggshell” osteotomy. J Neurosurg. 92(1suppl):50–56. 2000.6). Halm H, Metz-Stavenhagen P, Zielke K. Results of surgical correction of kyphotic deformities of the spine in ankylosing spondylitis on the basis of the modified arthritis impact measurement scales. Spine. 20:1612–1619. 1995.
Article7). Hehne HJ, Zielke K, Bohm H. Polysegmental lumbar osteotomies and transpedicled fixation for correction of long-curved kyphotic deformities in ankylosing spondylitis. Report on 177 cases. Clin Orthop. 258:49–55. 1990.8). Jaffray D, Becker V, Eisenstein S. Closing wedge osteotomy with transpedicular fixation in ankylosing spondylitis. Clin Orthop. 279:122–126. 1992.
Article9). Kim KT, Suk KS, Cho YJ, Hong KP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine. 27(6):612–618. 2002.
Article10). LaChapelle EH. Osteotomy of the lumbar spine for correction of kyphosis in a case of ankylosing spondylitis. J Bone Joint Surg. 28:851–858. 1946.11). Law WA. Osteotomy of the cervical spine: report of a case of ankylosing spondylitis. J Bone Joint Surg. 44-A:1199–1206. 1962.12). McMaster MJ. A technique for lumbar spinal osteotomy in ankylosing spondylitis. J Bone Joint Surg. 67-B:204–210. 1985.
Article13). Puschel J, Zielke K. Corrective surgery for kyphosis in Bekhterev's disease-Indication, technique, results. Z Orthop Ihre Grenzgeb. 120:338–342. 1982.14). Puschel J, Zielke K. Transpedicular vertebral instrumentation using VDS-instruments in ankylosing spondylitis. Orthopaedic Transactions. 9:130. 1985.15). Sengupta DK, Khazim R, Grevitt MP, Webb JK. Flexion osteotomy of the cervical spine: A new technique for correction of iatrogenic extension deformit in ankylosing spondylitis. Spine. 26(9):1068–1072. 2001.16). Simmons EH. Kyphotic deformity of the spine in ankylosing spondylitis. Clin Orthop. 128:65–77. 1977.
Article17). Smith-Petersen MN, Larson CB, Aufrand OE. Osteotomy of the spine for correction of flexion deformity in rheumatoid arthritis. J Bone Joint Surg. 27A:1–11. 1945.
Article18). Thiranont N, Netrawichien P. Transpedicular decancellation closed wedge vertebral osteotomy for treatment of fixed flexion deformity of spine in ankylosing spondylitis. Spine. 18:2517–2522. 1993.
Article19). Thomasen E. Vertebral osteotomy for correction of kyphosis in ankylosing spondylitis. Clin Orthop. 194:142–151. 1985.
Article20). von Royen BJ, Slot GM. Closing-wedge posterior osteotomy for ankylosing spondylitis. J Bone Joint Surg. 77-B:117–21. 1995.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multisegmental Osteotomy for Kyphotic Deformity in Ankylosing Spondylitis
- Ankylosing Spondylitis: Prevention And Surgical Correction Of Deformity
- Chin on Chest Deformity Caused by Upper Cervical Kyphosis Associated With Ankylosing Spondylitis: A Case Report
- Correction of kyphotic deformity in ankylosing spondylitis by posterior vertebral body decancellation: a case report
- Computer Simulation for Surgical Correction of Kyphotic Deformity in Ankylosing Spondylitis: A Narrative Review
