Determination of Distal Fusion Level with Segmental Pedicle Screw Fixation in Single Thoracic Idiopathic Scoliosis
- Affiliations
-
- 1Department of Orthopaedic Surgery. St. Paul's Hospital. Catholic University of Korea School of Medicine, Korea. dragon@sanggyepaik.ac.kr
- 2Seoul Spine Institute, Inje University Sanggye Paik Hospital, Korea.
Abstract
-
STUDY DESIGN: Retrospective study.
OBJECTIVES
To determine the exact distal fusion level in the treatment of single thoracic idiopathic scoliosis (King III and IV) with segmental pedicle screw fixation and rod rotation. SUMMARY OF LITERATURE REVIEW: Pedicle screw fixation effectively shortens the distal fusion extent by improved 3-D deformity correction. However, the selection of distal fusion extent remains controversial in single thoracic idiopathic scoliosis. MATERIAL AND METHODS: Forty-two single thoracic adolescent idiopathic scoliosis patients subject to segmental pedicle screw fixation and rod rotation with minimum follow-up of 2 years (2-6 years) were analyzed. The patients were grouped according to the distal fusion level with reference to the standing neutral vertebra (NV) for comparison of deformity correction, radiological and clinical spinal balance using standing radiographs. Distal fusion down to NV +1 was in 9 patients, NV in 5, NV-1 in 9, NV-2 in 12 and NV-3 in 7 patients respectively.
RESULTS
Preoperative 50+/-11 degrees of thoracic deformity was corrected to 13+/-5 degrees showing 74% of curve correction. Preoperative 23+/-7 degrees of lumbar deformity was corrected to 2+/-8 degrees showing 93% of curve correction. Postoperative adding on deformity was obtained in 14 patients. Significant difference was found not by King classification but by distal fusion level: significantly higher chance of unsatisfactory results from not going to the NV-1 (p=0.001).
CONCLUSIONS
In correction of single thoracic idiopathic scoliosis with segmental pedicle screw fixation, the curve should be fused to NV-1 saving one or more motion segments when compared to the fusion to the stable vertebra.
Keyword
MeSH Terms
Figure
-

Fig. 1-A. Preoperative standing anteroposterior radiograph of a 15.8 year old female with 50。 thoracic and 32。 lumbar fractional curve. As determined by the spinous process and pedicle shadows, the neutral vertebrae was L1. Fig. 1-B. Preoperative standing lateral radiograph. Fig. 1-C. Anteroposterior radiograph taken 3.5 years after surgery. The distal fusion was down to neutral vertebra(NV). The thoracic curve is corrected to 10。 with 9。 lumbar fractional curve and balanced spine. Fig. 1-D. Lateral radiograph taken 3.5 years after surgery.
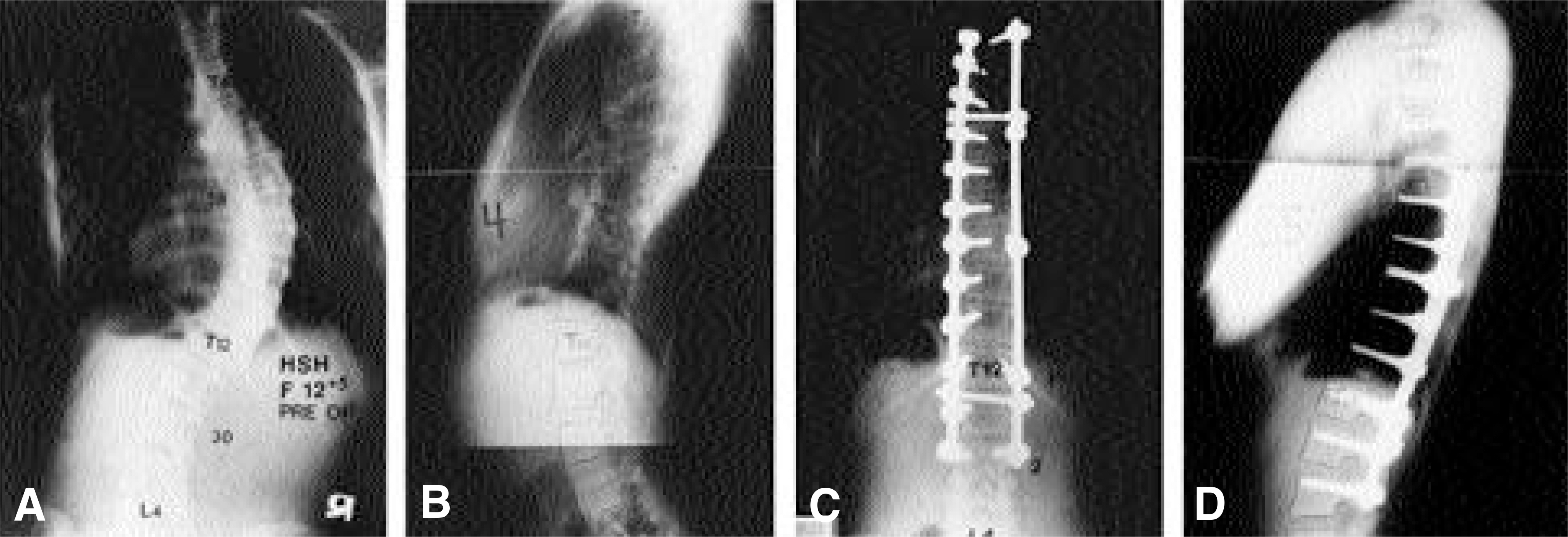
Fig. 2-A. Preoperative standing anteroposterior radiograph of a 12.4 year old female with 58。 thoracic and 30。 lumbar fractional curve. As determined by the spinous process and pedicle shadows, the neutral vertebrae was L3. Fig. 2-B. Preoperative standing lateral radiograph. The thoracic spine was hypokyphotic, 4。 of kyphosis. Fig. 2-C. Anteroposterior radiograph taken 4 years after surgery. The distal fusion was down to NV-1 (one level proximal to neutral vertebra). The thoracic curve is corrected to 3。 with 29。 lumbar fractional curve and balanced spine. Fig. 2-D. Lateral radiograph taken 4 years after surgery. The thoracic kyphosis was improved to 25。.
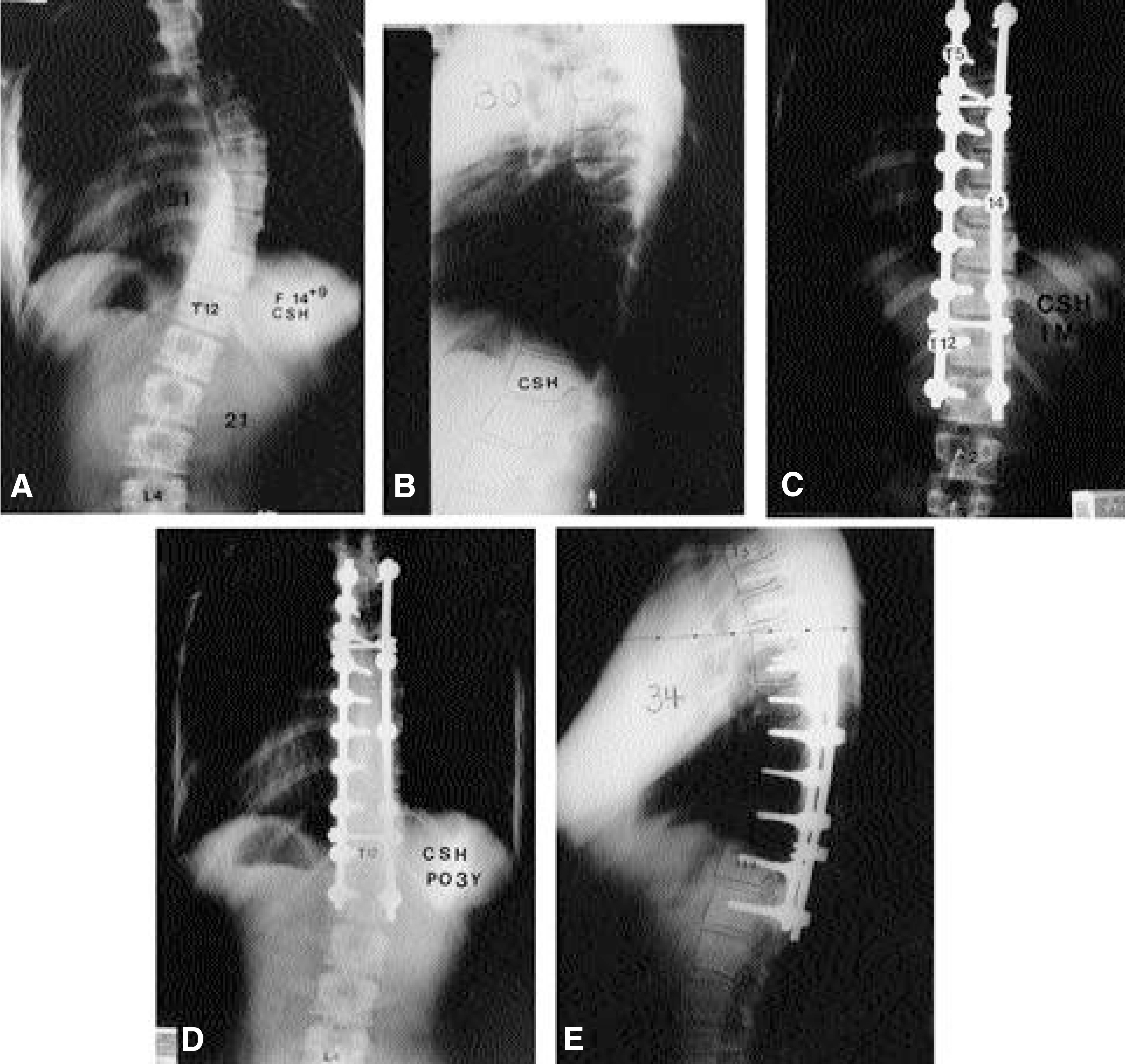
Fig. 3-A. Preoperative standing anteroposterior radiograph of a 14.8 year old female with 51。 thoracic and 21。 lumbar fractional curve. As determined by the spinous process and pedicle shadows, the neutral vertebrae was L3. Fig. 3-B. Preoperative standing lateral radiograph. Fig. 3-C. Anteroposterior radiograph taken 2 weeks after surgery. The distal fusion was down to NV-2 (two level proximal to neutral vertebra). The thoracic curve was corrected to 14。 with 2。 lumbar fractional curve and balanced spine. Fig. 3-D. Anteroposterior radiograph taken 3 years after surgery. The lumbar fractional curve shows reversal, resulting in extension of the index thoracic curve into the lumbar segments through adding on. Fig. 3-E. Lateral radiograph taken 3 years after surgery.
Reference
-
1). Arlet V, Marchesi D, Papin P, Aebi M. Decompensation following scoliosis surgery: treatment by decreasing the correction of the main thoracic curve of “ letting the spine go”. Eur spine J. 9:156–60. 2000.2). Benli IT, Tuzuner M, Akaline S, Kis M, Ayden E, Tandogan R. Spinal imbalance and decompensation problems in patients treated with Cotrel-Dubousset instru - mentation. Eur Spine J. 5:380–6. 1996.3). Bridwell KH, McAllister JW, Betz RR, Huss G, Clancy M, Schoenecker PL. Coronal decompensation produced by Cotrel-Dubousset “derotat ion” maneuver for idiopathic right thoracic scoliosis. Spine. 16:769–77. 1991.4). Cochran T, Irstam L, Nachemson A. Long term anatomic and functional changes in patients with adolescent idiopathic scoliosis treated by Harrington rod fusion. Spine. 8:576–84. 1983.5). Cotrel Y, Dubousset J, Guillaumat M. New universal instrumentation in spinal surgery. Clin Orthop, Feb;. 227:10–23. 1988.
Article6). King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg [Am]. 65:1302–13. 1983.
Article7). Lenke LG, Betz RR, Bridwell KH, Harms J, Clements DH, Lowe TG. Spontaneous lumbar curve coronal correction after selective anterior or posterior thoracic fusion in adolescent idiopathic scoliosis. Spine. 24:1663–71. 1999.
Article8). Lenke LG, Bridwell KH, Baldus C, Blanke K, Schoenecker PL. Cotrel-dubousset Instrumentation for Adolescent idiopathic Scoliosis. J Bone Joint Surg [Am]. 74:1056–67. 1992.
Article9). Margulies JY, Floman Y, Robin GC, Neuwirth MG, Kuflik P, Weidenbaum M, Farcy JP. An algorithm for selection of instrumentation levels in scoliosis. Eur Spine J. 7:88–94. 1998.
Article10). Mason DE, Carango P. Spinal decompensation in Cotrel-Dubousset instrumentation. Spine. 8:S394–403. 1991.
Article11). Moore MR, Baynham GC, Brown CW, Donaldson DH, Odom JA Jr. Analysis of factors related to truncal decompensation following Cotrel-Dubousset instrumentation. J Spinal Disord. 4:188–92. 1991.
Article12). Suk SI, Kim JH, Kim WJ, Lee SM, Liu Yi, Lee CS, Chung ER, Yoon YS. Restoration of thoracic kyphosis in idiopathic scoliosis - A comparison between multiple hook and segmental pedicle screw fixation in adolescent idiopathic scoliosis(AIS). J of Korean Spine Surg. 5:184–92. 1998.13). Suk SI, Lee CK, Kim WJ, Park YB, Chung YJ, Song KY. Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. J of Korean Orthop Assoc. 30:49–58. 1995.
Article14). Suk SI, Kim WJ, Lee SM, Kim JH, Chung ER. Thoracic pedicle screw fixation in spinal deformities. Are they really safe Spine. 26:2049–57. 2001.
Article15). Shufflebarger HL, Clark CE. Fusion levels and hook patterns in thoracic scoliosis with Cotrel-Dubousset instrumentation. Spine. 15:916–20. 1990.
Article16). Thompson JP, Transfeldt EE, Bradford DS, Ogilvie JW, Bouchie-Adjei O. Decompensation after Cotrel-Dubousset instrumentation of idiopathic scoliosis. Spine. 15:927–31. 1990.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Results of Selective Thoracic Fusion by Segmental Pedicle Screws in King type II Adolescent Idiopathic Scoliosis ( AIS )
- The Influence of Segmental Pedicle Screw Fixation on Distal Fusion Level in KingType I Adolescent Idiopathic Scoliosis(AIS)
- Selective Thoracic Fusion with Segmental Pedicle Screw Fixation for the Treatment of Thoracic Idiopathic Scoliosis: More than Five Year's Follow-Up
- Segmental pedicle screw fixation in the treatment of Thoracic idiopathic scoliosis
- Decompensation in Selective Thoracic Fusion by Segmental Pedicle Screw Fixation in King type II Adolescent Idiopathic Scoliosis (AIS): Causative Factors and its Prevention
