Intra-Arterial Thrombolysis for Deep Vein Thrombosis of the Lower Extremity: Case Report
- Affiliations
-
- 1Department of Radiology, Wonkwang University School of Medicine, Iksan, Korea. bsroh@wonkwang.ac.kr
Abstract
- If the appropriate catheterization of the affected vein was not possible because of a narrowed or thrombus-filled venous lumen, successful treatment gets into trouble during catheter directed regional thrombolysis for treatment of deep vein thrombosis. In this situation, intra-arterial thrombolysis can be considered as an alternative treatment, but to the best of our knowledge, only two reports have been described. We present here cases of successful intra-arterial thrombolysis in patients with deep vein thrombosis.
MeSH Terms
Figure
-
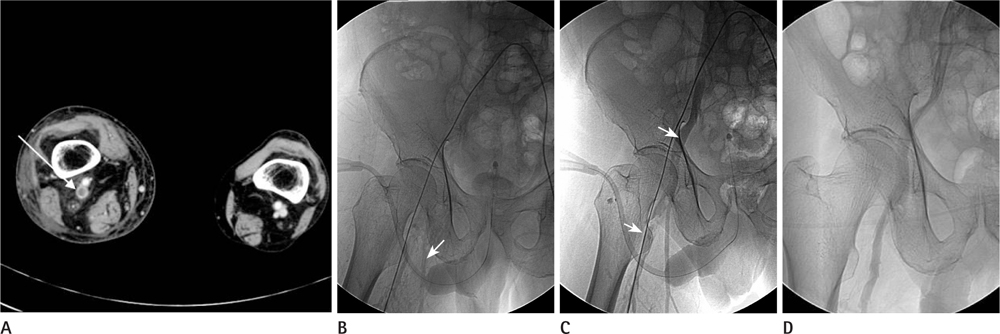
Fig. 1 67-year-old male with deep vein thrombosis of the right lower extremity. A. CT angio venography showed thrombotic occlusion of right femoral vein (arrow). Catheterization into popliteal vein was failed due to narrowed, thrombus-filled lumen. Alternatively, infusion catheter was located into the right popliteal artery. Catheter-directed thrombolysis with urokinase (50,000 IU/hr) was attempted. B. Initial Venography showed nearly obliterated right iliofemoral vein. Venous drainage of deep femoral and saphenous vein was relatively prominent (arrow). C. After 44 hours of urokinase infusion, venography showed patency of iliofemoral segment (arrow). D. Follow up venography showed good patency of right iliofemoral and popliteal veins after 7 days.
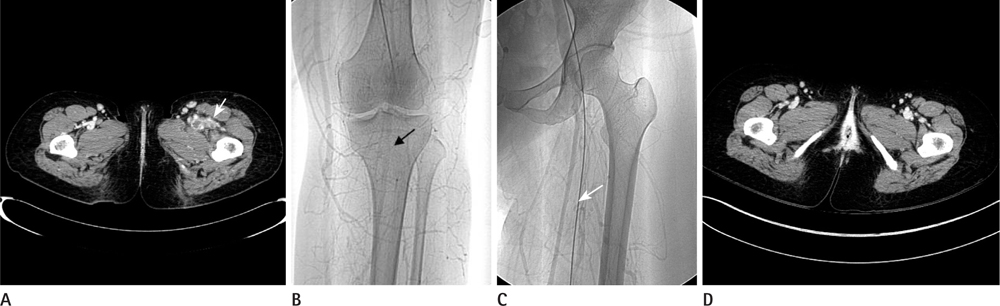
Fig. 2 33-year-old female with deep vein thrombosis of the left lower extremity. A. CT angio venography showed multiple thrombotic occlusion of left femoral, popliteal and tibial veins with enhanced thick wall and collapsed lumen (arrow). B, C. After 2 days of urokinase infusion, venography showed faint drainage flow of superficial femoral and popliteal veins (arrow). D. Follow-up CT angio venography after 3.5 years showed good patency of both iliofemoral and popliteal veins.
Reference
-
1. Sharafuddin MJ, Sun S, Hoballah JJ, Youness FM, Sharp WJ, Roh BS. Endovascular management of venous thrombotic and occlusive diseases of the lower extremities. J Vasc Interv Radiol. 2003; 14:405–423.2. Lee KH, Han H, Lee KJ, Yoon CS, Kim SH, Won JY, et al. Mechanical thrombectomy of acute iliofemoral deep vein thrombosis with use of an Arrow-Trerotola percutaneous thrombectomy device. J Vasc Interv Radiol. 2006; 17:487–495.3. Roh BS. Endovascular management of deep venous thrombotic diseases of the lower extremity. J Korean Radiol Soc. 2004; 51:1–12.4. Wlodarczyk ZK, Gibson M, Dick R, Hamilton G. Low-dose intra-arterial thrombolysis in the treatment of phlegmasia caerulea dolens. Br J Surg. 1994; 81:370–372.5. Garg SK, Yadav KS. Developing venous gangrene in deep vein thrombosis: intraarterial low-dose burst therapy with urokinase--case reports. Angiology. 1999; 50:157–162.6. Henao EA, Bohannon WT, Silva MB Jr. Treatment of portal venous thrombosis with selective superior mesenteric artery infusion of recombinant tissue plasminogen activator. J Vasc Surg. 2003; 38:1411–1415.7. Paques M, Vallée JN, Herbreteau D, Aymart A, Santiago PY, Campinchi-Tardy F, et al. Superselective ophthalmic artery fibrinolytic therapy for the treatment of central retinal vein occlusion. Br J Ophthalmol. 2000; 84:1387–1391.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Upper Extremity Deep Vein Thrombosis after Clavicle Fracture and Immobilization
- The Incidence of Deep Vein Thrombosis in the Lower Extremity
- A Case of Upper Extremity Deep Vein Thrombosis and Pulmonary Thromboembolism in a Severely Obese Man
- Vascular Interventional Procedures Often Encountered by Primary Physicians
- Catheter Directed Thrombolysis for Deep Vein Thrombosis during the First Trimester of Pregnancy: Two Case Reports
