J Korean Acad Oral Health.
2013 Dec;37(4):194-199.
Impact of amalgam removal on urinary mercury concentration in children: a pilot study
- Affiliations
-
- 1Department of Preventive Dentistry, Kyungpook National University School of Dentistry, Daegu, Korea. cyh1001@knu.ac.kr
Abstract
OBJECTIVES
This pilot study aimed to evaluate the effect of dental amalgam, a restorative material, on children by measuring the mercury concentration in the urine as well as the number of teeth filled with dental amalgam.
METHODS
Twenty children enrolled in grades 1-4 of two elementary schools in Daegu participated in this study. One trained dentist performed oral examinations and removed amalgam restorations from the teeth with a high and low speed handpiece. In order to measure the urinary mercury concentrations, urine samples were collected from all participants at baseline and immediately and 24 hours after removal of the dental amalgam restorations.
RESULTS
The mean number of teeth from which the amalgam restorations was removed was 9.8 while the mean urinary mercury concentrations at baseline, immediately, and 24 hours after removal of dental amalgam restorations were 2.66, 2.76, and 2.76 microg/g creatinine, respectively. The mean urinary mercury concentration increased consistently after amalgam restoration removal. For those participants whose removed amalgamated surfaces were more than 11, the mean urinary mercury concentration immediately after amalgam restoration removal and 24 hours after removal increased consistently but showed no significant difference.
CONCLUSIONS
This study demonstrated that dental amalgam restoration was related to urinary mercury concentration, and these findings present a possibility of mercury accumulation in the body. Therefore, we suggest future longitudinal studies to ensure the safety of children exposed to mercury by establishing criteria for amalgam removal.
MeSH Terms
Figure
-
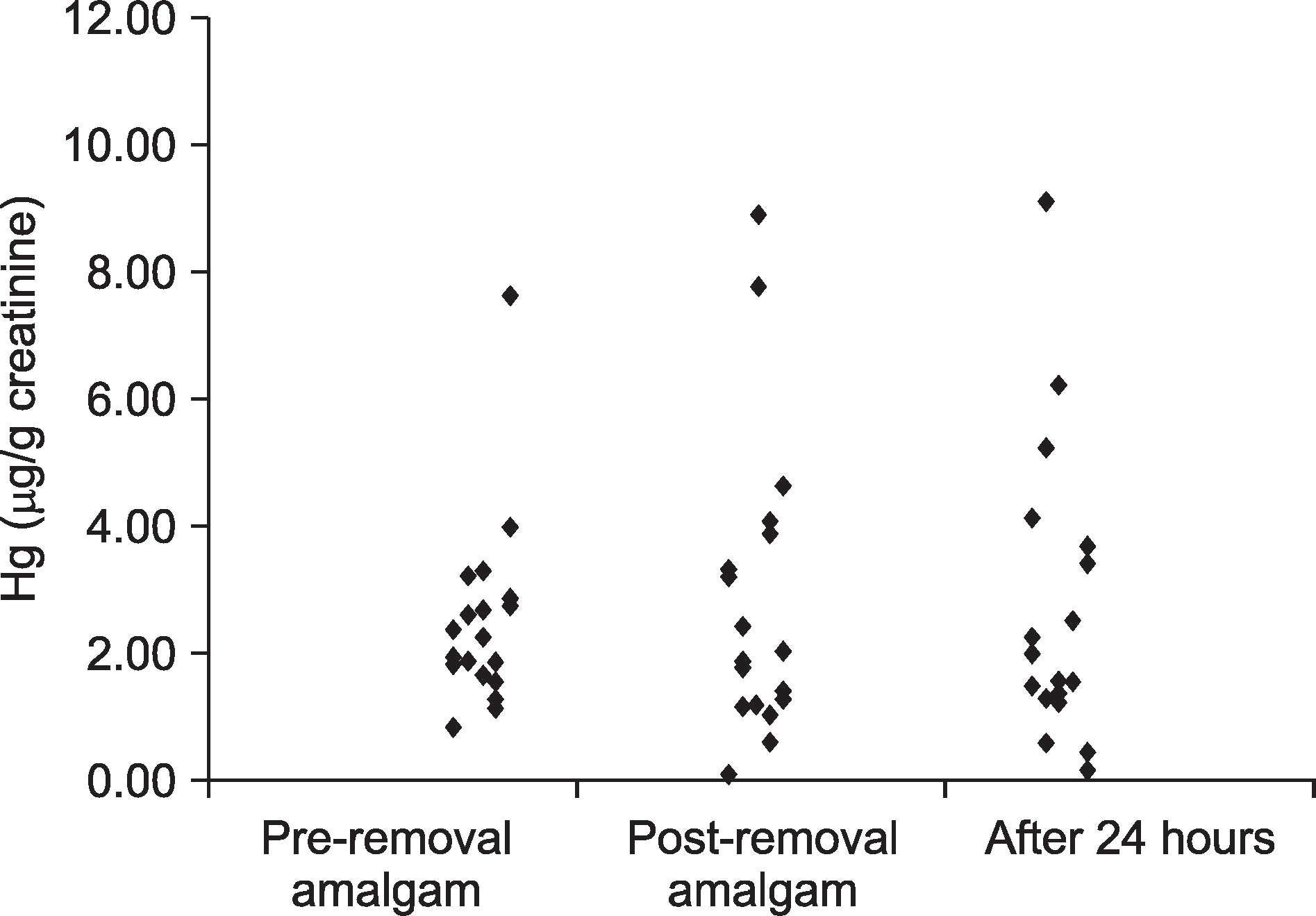
Fig. 1. Concentration urinary mercury according to the sampling times.
Reference
-
References
1. Marshall SJ, Marshall GW. Dental amalgam: the materials. Adv Dent Res. 1992; 6:94–99.
Article2. Fredén H, Helldén L, Milleding P. Mercury content in gingival tissues adjacent to amalgam fillings. Odontol Revy. 1974; 25:207–210.3. Hibberd JH, Smith DC. Systemic mercury levels in dental office personnel in Ontario: a pilot study. J Can Dent Assoc. 1972; 38:249–254.4. Fuks AB. The use of amalgam in pediatric dentistry. Pediatr Dent. 2002; 24:448–455.5. Needleman HL. Mercury in dental amalgam- a neurotoxic risk? JAMA. 2006; 295:1835–1836.6. Levy M, Schwartz S, Dijak M, Weber JP, Tardif R, Rouah F. Childhood urine mercury excretion: dental amalgam and fish consumption as exposure factors. Environ Res. 2004; 94:283–290.
Article7. Khordi-Mood M, Sarraf-Shirazi AR, Balali-Mood M. Urinary mercury excretion following amalgam filling in children. J Toxicol Clin Toxicol. 2001; 39:701–705.
Article8. WHO. Environmental Health Criteria 1: Mercury. Geneva: WHO;1976. p. 94–131.9. Joint FAO/WHO Expert Committee on Food Additives. WHO Technical Report Series 940. Geneva: World Health Organization;2006. p. 53–59.10. Counter SA, Buchanan LH. Mercury exposure in children: a review. Toxicol Appl Pharmacol. 2004; 198:209–230.
Article11. Jin HJ, Sa KJ, Choi YH, An SY, Lee YE, Song KB. Relationship between dental amalgam fillings and urinary mercury concentration among children. J Korean Acad Oral Health. 2011; 35:258–266.12. Berglund A, Molin M. Mercury vapor release from dental amalgam in patients with symptoms allegedly caused by amalgam fillings. Eur J Oral Sci. 1996; 104:56–63.
Article13. Molin M, Bergman B, Marklund SL, Schütz A, Skerfving S. Mercury, selenium, and glutathione peroxidase before and after amalgam removal in man. Acta Odontol Scand. 1990; 48:189–202.
Article14. Kremers L, Halbach S, Willruth H, Mehl A, Welzl G, Wack FX, et al. Effect of rubber dam on mercury exposure during amalgam removal. Eur J Oral Sci. 1999; 107:202–207.
Article15. Arndt T. Urine-creatinine concentration as a marker of urine dilution: Reflections using a cohort of 45,000 samples. Forensic Sci Int. 2009; 186:48–51.
Article16. Ohira S, Kirk AB, Dasgupta PK. Automated measurement of urinary creatinine by multichannel kinetic spectrophotometry. Anal Biochem. 2009; 384:238–244.
Article17. Schulz C, Angerer J, Ewers U, Heudorf U, Wilhelm M. Revised and new reference values for environmental pollutants in urine or blood of children in Germany derived from the German environmental survey on children 2003-2006 (GerES IV). Int J Hyg Environ Health. 2009; 212:637–647.
Article18. Caldwell KL, Mortensen ME, Jones RL, Caudill SP, Osterloh JD. Total blood mercury concentrations in the U. S. population: 1999-2006. Int J Hyg Environ Health. 2009; 212:588–598.19. Ewers U, Krause C, Schulz C, Wilhelm M. Reference values and human biological monitoring values for environmental toxins. Report on the work and recommendations of the Commission on Human Biological Monitoring of the German Federal Environmental Agency. Int Arch Occup Environ Health. 1999; 72:255–260.20. Agency for Toxic Substance and Disease Registry. Toxicological profile for mercury. Atlanta: US Department of health and human service;1999.21. Olstad ML, Holland RI, Wandel N, Pettersen AH. Correlation between amalgam restorations and mercury concentrations in urine. J Dent Res. 1987; 66:1179–1182.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mercury exposure from dental amalgam: a 6 month follow-up
- Two Cases of Mercury Dermatitis Following Amalgam Dental Restorations
- The Relationship Between Amalgam Tooth Fillings and Concentration of Blood Mercury in Elementary School Students in Korea
- Association between dental amalgam restoration and urine mercury concentrations among young women: a cross-sectional study
- Mercury Concentration in air and in Urine of Workers in Fluorescent Lamp Manufacturing Factories in Korea
