J Korean Acad Oral Health.
2013 Sep;37(3):154-160.
Trends in oral health inequality in 12-year-old Korean children: A study using the Gini coefficient
- Affiliations
-
- 1Research Institute for Dental Care Policy, Korean Dental Association, Seoul, Korea. yulsaram@naver.com
Abstract
OBJECTIVES
This study was conducted to analyze the current state and tendency of oral health inequality in 12-year-old Korean children by calculating the Gini coefficient from decayed, missing, or filled teeth (DMFT) data.
METHODS
Ten-year trends were empirically estimated by calculating the Gini coefficient from the Lorenz curve plotted based on the DMFT data of 12-year-old children, obtained from the Korean National Oral Health Survey from 2000 to 2010.
RESULTS
While the oral health improved in general, oral health inequalities increased with the decrease in the number of DMFT each year, and the DMFT-based Gini coefficient increased from 0.53 in 2000 to 0.61 in 2010. The increase in the number of decayed and missing teeth was strongly affected by the increase in oral health inequality.
CONCLUSIONS
To resolve Korea's continually increasing oral health inequality, it is necessary to establish support measures for vulnerable populations and to develop and manage a surveillance system for continuous monitoring of oral health inequality in the future.
Keyword
Figure
-
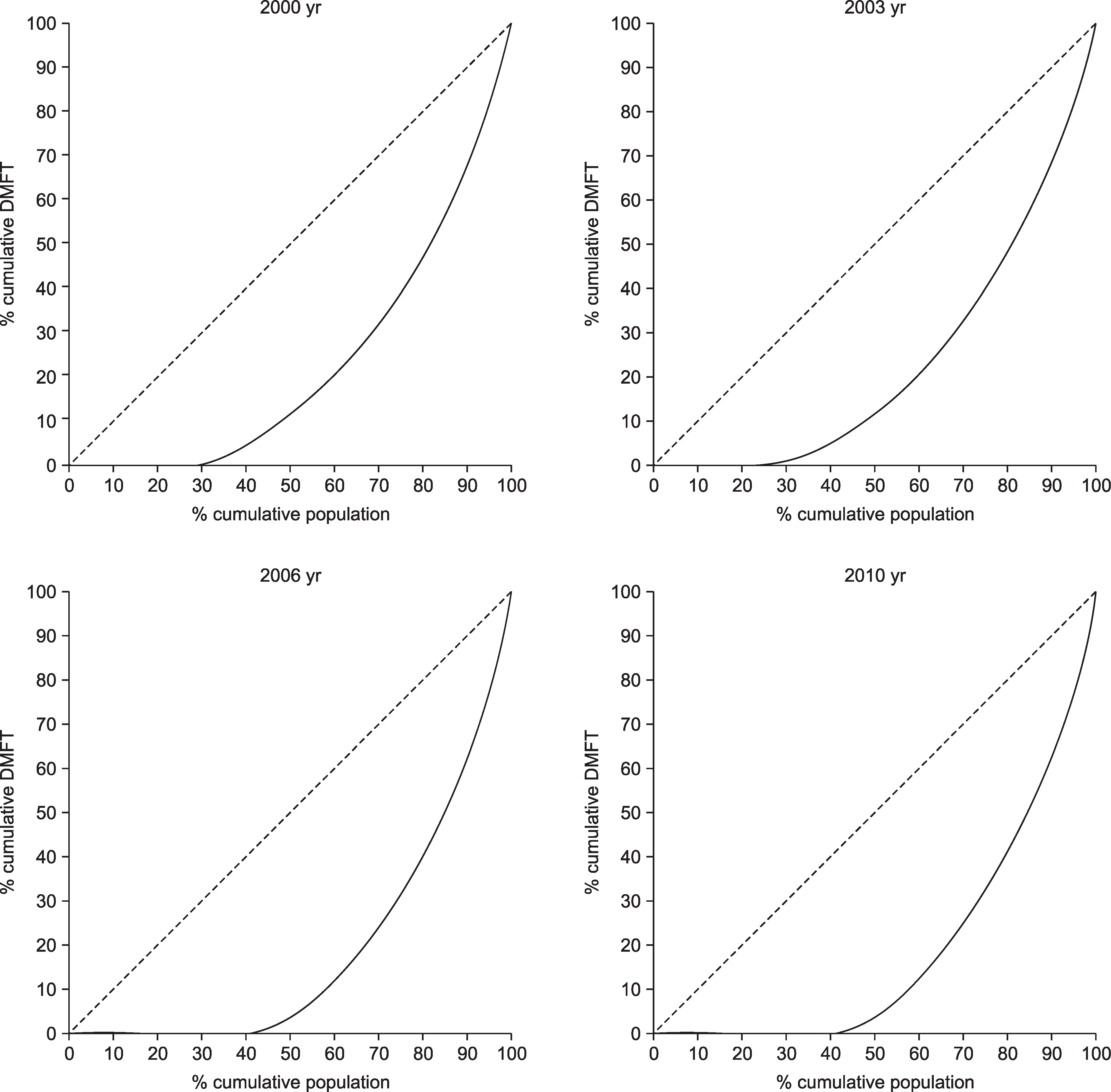
Fig. 1. Lorenz curves of DMFT for 12-year-old.

Fig. 2. Change of Gini coefficient of DMFT, DT+MT, FT.
Reference
-
References
1. University of Ulsan College of Medicine. Developing indicators of equity in health and monitoring magnitude of socioeconomic inequality in health. Seoul: Management Center for Health Pro-motion;2006. p. 28–31.2. Industry-University Cooperation Foundation Hanyang University. 2009 Korea Health Inequality Statistics. Seoul: Management Center for Health Promotion;2009. p. 16–23.3. Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Geneva: Commission on Social Determinants of Health;2008. p. 1–23.4. Oakes JM, Kaufman JS. Methods in Social Epidemiology. San Francisco: Jossey-Bass;2006. p. 134–168.5. Park HJ, Lee JH. The effect of socioeconomic status, oral health consciousness and behaviors on the periodontal-health disparities among Korean adults. Korean J Health Educ Promot. 2010; 27:61–69.6. Shin BM, Jung SH. Socio-economic inequalities in tooth loss and chewing difficulty in the Korean elderly. J Korean Acad Oral Health. 2012; 36:195–202.7. Shin HS. Kim HD. Income related inequality of dental care utilization in Korea. Health and Social Welfare Review. 2006; 26:69–93.8. Shin BM. A comparison of methods for measuring inequalities in oral health [dissertation]. Gangwon: Gangneung-Wonju National University;2013. [Korean].9. Locker D. Deprivation and oral health: a review. Community Dent Oral Epidemiol. 2000; 28:161–169.
Article10. Ravaghi V, Quinonez C, Allison PJ. The magnitude of oral health inequalities in Canada: findings of the Canadian health measures survey. Community Dent Oral Epidemiol. 2013; 5:1–9.
Article11. Do LG, Spencer AJ, Slade GD, Ha DH, Roberts-Thomson KF, Liu P. Trend of income-related inequality of child oral health in Australia. J Dent Res. 2010; 89:959–964.
Article12. Blair YI, Mcmahon AD, Macpherson LM. Comparison and relative utility of inequality measurements: as applied to Scotland’s child dental health. PLOS one. 2013; 8:1–9.
Article13. Jagger DC, Sherriff A, Macpherson LM. Measuring socio-economic inequalities in edentate Scottish adults-cross sectional analyses using Scottish Health Surveys 1995-2008/09. Community Dent Oral Epidemiol. 2013; 11:1–10.14. Ministry of Health and Welfare. Health plan 2020. Seoul: Ministry of Health and Welfare;2011. p. 320–351.15. Ministry of Health and Welfare. 2000 Korean National Oral Health Survey. Seoul: Ministry of Health and Welfare;2001. p. 1–4.16. Ministry of Health and Welfare. 2003 Korean National Oral Health Survey. Seoul: Ministry of Health and Welfare;2003. p. 1–14.17. Ministry of Health and Welfare. 2006 Korean National Oral Health Survey. Seoul: Ministry of Health and Welfare;2007. p. 1–10.18. Ministry of Health and Welfare. 2010 Korean National Oral Health Survey. Seoul: Ministry of Health and Welfare;2010. p. 1–13.19. Poulsen S, Heidmann J, Vaeth M. Lorenz curves and their use in describing the distribution of ‘the total burden’ of dental caries in a population. Community Dental Health. 2001; 18:68–71.20. Shkolnikov VM, Andreev EE, Begun AZ. Gini coefficient as a life table function: computation from discrete data, decomposition of differences and empirical examples. Demogr Res. 2003; 8:305–358.
Article21. Shin YJ, Kim MH, Jeon HJ, Kim SH. Social epidemiology. Seoul: Hanul publishing group;2003. p. 109–117.22. Ziebarth N. Measurement of health, health inequality, and reporting heterogeneity. Soc Sci Med. 2010; 71:116–124.
Article23. Ministry of Health and Welfare. 2013 Community integrated health promotion service. Seoul: Ministry of Health and Welfare Division of Healthy life and Oral health;2013. p. 1–95.24. Piovesan C, Mendes FM, Antunes JL, Ardenghi TM. Inequalities in the distribution of dental caries among 12-year-old Brazilian schoolchildren. Braz Oral Res. 2011; 25:69–75.
Article25. Armfield JM, Spencer AJ, Slade GD. Changing inequalities in the distribution of caries associated with improving child oral health in Australia. J Public Health Dent. 2009; 69:125–134.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Inequality in Private Health Care Expenditures: A 36-Year Trend Study of Iranian Households
- Alcohol-related emergency department visits and income inequality in New York City, USA: an ecological study
- Analysis of inequality trends in self-rated oral health and oral health-related quality of life of adults according to household income level using data from the Korea National Health and Nutrition Examination Survey
- Corrigendum: analysis of inequality trends in self-rated oral health and oral health-related quality of life of adults according to household income level using data from the Korea National Health and Nutrition Examination Survey
- Geographic Distribution of Physician Manpower by Gini Index
