World J Mens Health.
2012 Dec;30(3):198-201.
Metastatic Squamous Cell Carcinoma of the Kidney from Cholangiocarcinoma
- Affiliations
-
- 1Department of Urology, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea. urobae@genetherapy.or.kr
- 2Department of Urology, Andong Hospital, Andong, Korea.
Abstract
- We present a rare case of a metastatic renal tumor originating from adenosquamous carcinoma of the intrahepatic bile duct. A 64-year-old man treated with bisegmentectomy and extended cholecystectomy for cholangiocarcinoma had a left cystic renal mass, which had irregular wall thickening, heterogeneously low attenuation, and soft tissue infiltration as determined by a computed tomography scan. The first impression was renal abscess. Left nephrectomy was performed and the nonencapsulated mass was gray in color macroscopically. Histological examination of the specimen revealed alveolar proliferation of small cancer cells, which was consistent with the original tumor of the intrahepatic bile duct. The left renal tumor was misdiagnosed as a renal abscess but finally diagnosed as squamous cell carcinoma metastasized from the intrahepatic bile duct. The patient expired because of lung metastasis after 14 months following left nephrectomy. In our opinion, this case would be the first report of a renal metastasis from a cholangiocarcinoma clinically and was treated with nephrectomy.
MeSH Terms
Figure
-

Fig. 1 Left cystic renal mass with irregular wall thickening, heterogeneous attenuation, and soft tissue infiltration.
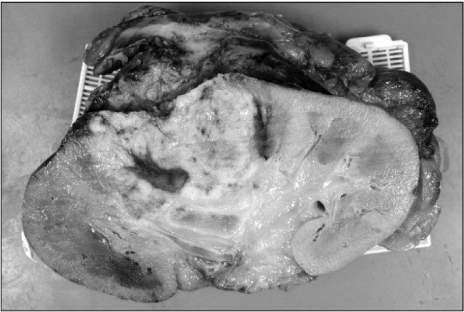
Fig. 2 Tumor is located in the renal pelvis, and extending to and infiltrating the renal parenchyma.
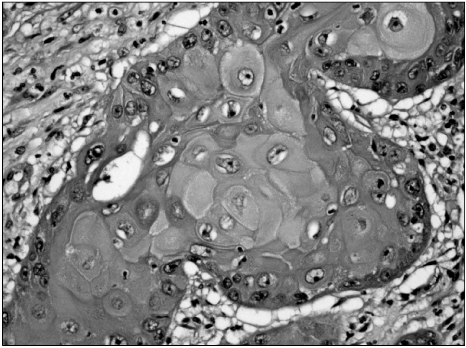
Fig. 3 Moderate-differentiated squamous cell carcinoma. Nests of infiltrating squamous cells with hyperchromatic nuclei and prominent keratin production should be noted (H&E, ×400).
Reference
-
1. Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. 1950. 3:74–85.2. Bracken RB, Chica G, Johnson DE, Luna M. Secondary renal neoplasms: an autopsy study. South Med J. 1979. 72:806–807.3. Mayer RJ. Rieselbach RE, Garnick MB, editors. Infiltrative and metastatic disease of the kidney. Cancer and the kidney. 1982. Philadelphia: Lea & Febiger;707.4. Sánchez-Ortiz RF, Madsen LT, Bermejo CE, Wen S, Shen Y, Swanson DA, et al. A renal mass in the setting of a nonrenal malignancy: When is a renal tumor biopsy appropriate? Cancer. 2004. 101:2195–2201.5. Peterson RO. Urologic pathology. 1992. Philadelphia: Lippincott;127.6. Wagle DG, Moore RH, Murphy GP. Secondary carcinomas of the kidney. J Urol. 1975. 114:30–32.
Article7. Choyke PL, White EM, Zeman RK, Jaffe MH, Clark LR. Renal metastases: clinicopathologic and radiologic correlation. Radiology. 1987. 162:359–363.
Article8. Rybicki FJ, Shu KM, Cibas ES, Fielding JR, vanSonnenberg E, Silverman SG. Percutaneous biopsy of renal masses: sensitivity and negative predictive value stratified by clinical setting and size of masses. AJR Am J Roentgenol. 2003. 180:1281–1287.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Metastatic Cutaneous Squamous Cell Carcinoma Arising in Chronic Osteomyelitic Focus
- A Case of Squamous Cell Carcinoma of Cervical Esophagus with Metastasis to Thyroid Gland
- Case report: simultaneous squamous cell carcinoma of uterine cervix and renal cell carcinoma of kidney
- Squamous Cell Carcinoma of the Renal Pelvis: A Case Report
- Fine Needle Aspiration Cytology of Metastatic Adenocarcinoma of Thyroid Gland from the Colon: Report of A case
