A Case of Significant Endobronchial Injury due to Recurrent Iron Pill Aspiration
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. drterry@hanyang.ac.kr
- 2Department of Pathology, Hanyang University College of Medicine, Seoul, Korea.
- KMID: 2320724
- DOI: http://doi.org/10.4046/trd.2015.78.4.440
Abstract
- Gastric mucosal damage by iron pills is often reported. However, iron pill aspiration is uncommon. Oxidation of the impacted iron pill causes bronchial mucosal damage that progresses to chronic bronchial inflammation, necrosis, endobronchial stenosis and rarely, perforation. We reported a case of a 92-year-old woman with chronic productive cough and significant left-sided atelectasis. Bronchoscopy revealed substantial luminal narrowing with exudative inflammation of the left main bronchus. Bronchial washing cytology showed necroinflammatory exudate and a small amount of brown material. Mucosal biopsy showed diffuse brown pigments indicative of ferrous pigments, crystal deposition, and marked tissue degeneration. After vigorous coughing, she expectorated dark sediments and her symptoms and radiological abnormalities improved. There are a few such reports worldwide; however, this was the first case reported in Korea. Careful observation of aspiration-prone patients and early detection of iron pill aspiration may prevent iron pill-induced bronchial injury.
Keyword
MeSH Terms
Figure
-
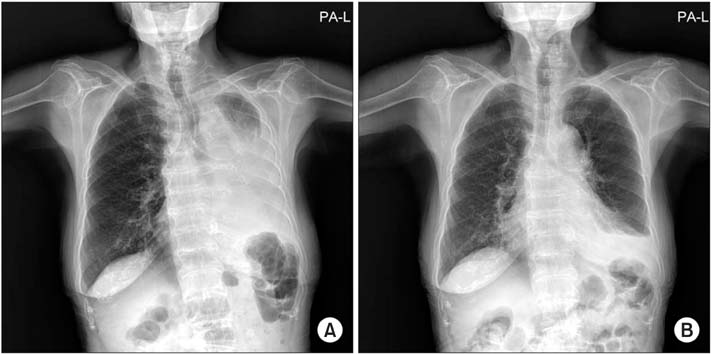
Figure 1 (A) At admission, chest radiograph shows near total atelectasis of the left lung and a large amount of pleural effusion in the left hemithorax. (B) On the fifth hospital day, chest radiograph reveals clear overall lung field with improved atelectasis and decreased effusion.
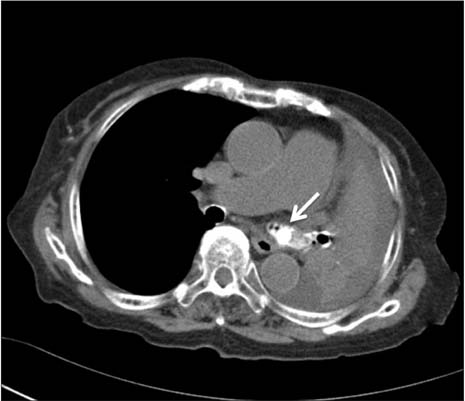
Figure 2 Chest computed tomography images show near total atelectasis of left lung and a dense calcified nodular lesion (arrow) impacted at the left main bronchus.

Figure 3 (A-D) Bronchoscopy shows substantial narrowed proximal portion of left main bronchus with irregular mucosal changes and brown, tarry exudative surface. LLL: left lower lobe; LUL: left upper lobe.

Figure 4 (A-C) Bronchial mucosal tissue showed marked necrosis and degeneration with diffusely scattered golden-yellow pigments (A, H&E stain, ×200; B, H&E stain, ×400, arrows). The tissue was stained entirely dark blue with Prussian blue (C, ×100).
Reference
-
1. Hill SN, Main AN, Fuggle WJ. Covert inhalation of tablet causing fatal pneumonia. Postgrad Med J. 1988; 64:66–67.2. Tarkka M, Anttila S, Sutinen S. Bronchial stenosis after aspiration of an iron tablet. Chest. 1988; 93:439–441.3. Lamaze R, Trechot P, Martinet Y. Bronchial necrosis and granuloma induced by the aspiration of a tablet of ferrous sulphate. Eur Respir J. 1994; 7:1710–1711.4. Cimino-Mathews A, Illei PB. Cytologic and histologic findings of iron pill-induced injury of the lower respiratory tract. Diagn Cytopathol. 2013; 41:901–903.5. Delgado-Sanchez L, Atwal P, Krishnan P. Iron pill induced bronchitis. Int J Case Rep Imag. 2012; 3:34–36.6. Lee P, Culver DA, Farver C, Mehta AC. Syndrome of iron pill aspiration. Chest. 2002; 121:1355–1357.7. Godden DJ, Kerr KM, Watt SJ, Legge JS. Iron lung: bronchoscopic and pathological consequences of aspiration of ferrous sulphate. Thorax. 1991; 46:142–143.8. Aust SD, Morehouse LA, Thomas CE. Role of metals in oxygen radical reactions. J Free Radic Biol Med. 1985; 1:3–25.9. Kim ST, Kaisar OM, Clarke BE, Vandenburg RA, Allen DH, Bell SC, et al. 'Iron lung': distinctive bronchoscopic features of acute iron tablet aspiration. Respirology. 2003; 8:541–543.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Photodynamic Therapy for Endobronchial Obstruction due to Recurrent Lung Cancer : 2 Cases Report
- Severe Endobronchial Inflammation Induced by Aspiration of a Ferrous Sulfate Tablet
- A case of bronchomalacia due to endobronchial tuberculosis
- A Case of Hair Structure Abnormality Associated with Iron Deficiency Anaemia
- Penetrating Injury by an Iron Reinforcing Bar Associated with a Fall or Slip Injury
