Aberrant Bronchial Artery to Non-Sequestrated Left Upper Lobe in Massive Hemoptysis
- Affiliations
-
- 1Department of Internal Medicine, Chonbuk National University Hospital, Jeonju, Korea. cough@jbnu.ac.kr
- 2Department of Radiology, Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 2320711
- DOI: http://doi.org/10.4046/trd.2015.78.4.380
Abstract
- Systemic arterial supply from the descending thoracic aorta to the basal segment of the left lower lobe without a pulmonary arterial supply is a rare congenital anomaly within the spectrum of sequestration lung disease. The most common pattern of anomalous systemic artery to the lung arises from the descending thoracic aorta and feeds the basal segments of the left lower lobe. We report an extremely rare case of a 29-year-old woman who underwent a successful left upper lobectomy for the treatment of recurrent massive hemoptysis from anomalous bronchial arterial supply to the lingular segment of left upper lobe.
MeSH Terms
Figure
-

Figure 1 Selective bronchial angiograms reveal a hypertrophied bronchial artery (A) and vascular staining (B) in the apico-posterior segment of the left upper lobe.
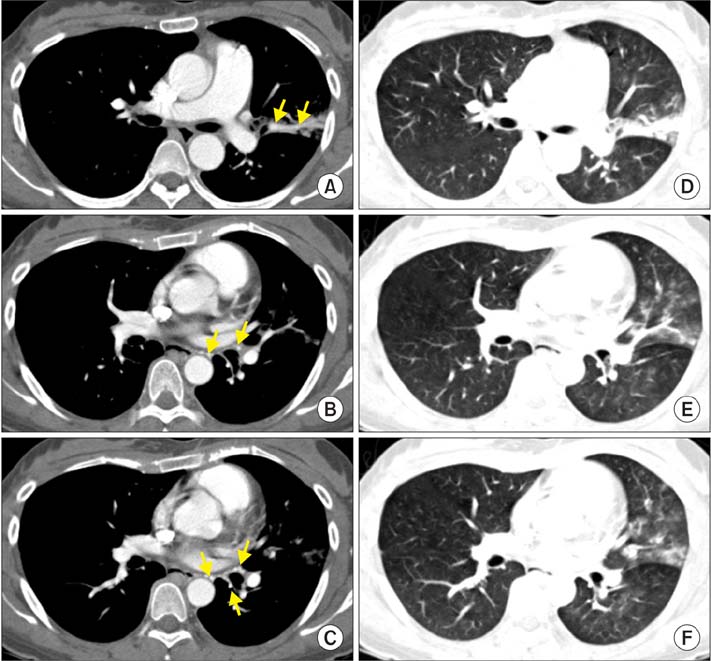
Figure 2 Anomalous systemic arterial supply to normal lung parenchyma in a 29-year-old woman with recurrent hemoptysis. Multidetector computed tomographic angiography in mediastinal window settings (A-C) shows multiple nodular and curvilinear structures with high attenuation within the mediastinal soft tissue (arrows in A-C) and left upper lobe that indicate systemic arteries. In lung window settings (D-F), scans showed hypertrophied vessels in the left upper lobe and ground-glass attenuation in the left upper lobe and left lower lobe that is probably due to hyperemia from systemic supply to the lung and aspirated blood.
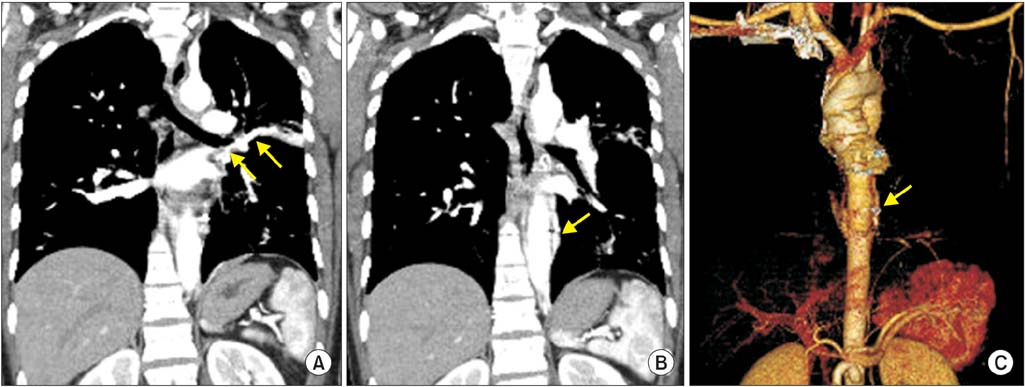
Figure 3 A coronal computed tomography (CT) image (A) shows aberrant bronchial artery (arrows in A) supplying the left upper lobe. After identifying aberrant bronchial artery in the CT and bronchial angiogram, bonchial artery embolization was performed to control hemoptysis in this patient. A coronal (B) and a volume-rendered CT image (C) reveal embolization coils (arrows in B and C) at the proximal portion of aberrant bronchial artery.
Reference
-
1. Cauldwell EW, Siekert RG. The bronchial arteries; an anatomic study of 150 human cadavers. Surg Gynecol Obstet. 1948; 86:395–412.2. Hiramatsu M, Iwashita M, Inagaki T, Matsudaira H, Hirano J, Odaka M, et al. Anomalous systemic arterial supply to separate lingular and basal segments of the lung: an anatomic consideration. Ann Thorac Surg. 2009; 88:1358–1360.3. Albertini A, Dell'Amore A, Tripodi A, Del Giglio M, Pagliaro M, Calvi S, et al. Anomalous systemic arterial supply to the left lung base without sequestration. Heart Lung Circ. 2008; 17:505–507.4. Cohen AM, Antoun BW, Stern RC. Left thyrocervical trunk bronchial artery supplying right lung: source of recurrent hemoptysis in cystic fibrosis. AJR Am J Roentgenol. 1992; 158:1131–1133.5. Sade RM, Clouse M, Ellis FH Jr. The spectrum of pulmonary sequestration. Ann Thorac Surg. 1974; 18:644–658.6. Sancho C, Escalante E, Dominguez J, Vidal J, Lopez E, Valldeperas J, et al. Embolization of bronchial arteries of anomalous origin. Cardiovasc Intervent Radiol. 1998; 21:300–304.7. Flisak ME, Chandrasekar AJ, Marsan RE, Ali MM. Systemic arterialization of lung without sequestration. AJR Am J Roentgenol. 1982; 138:751–753.8. Battal B, Akgun V, Karaman B, Bozlar U, Tasar M. Normal anatomical features and variations of bronchial arteries: an analysis with 64-detector-row computed tomographic angiography. J Comput Assist Tomogr. 2011; 35:253–259.9. Khalil A, Parrot A, Nedelcu C, Fartoukh M, Marsault C, Carette MF. Severe hemoptysis of pulmonary arterial origin: signs and role of multidetector row CT angiography. Chest. 2008; 133:212–219.10. Deffebach ME, Charan NB, Lakshminarayan S, Butler J. The bronchial circulation. Small, but a vital attribute of the lung. Am Rev Respir Dis. 1987; 135:463–481.11. Osiro S, Wear C, Hudson R, Ma XX, Zurada A, Michalak M, et al. A friend to the airways: a review of the emerging clinical importance of the bronchial arterial circulation. Surg Radiol Anat. 2012; 34:791–798.12. Do KH, Goo JM, Im JG, Kim KW, Chung JW, Park JH. Systemic arterial supply to the lungs in adults: spiral CT findings. Radiographics. 2001; 21:387–402.13. Tao CW, Chen CH, Yuen KH, Huang MH, Li WY, Perng RP. Anomalous systemic arterial supply to normal basilar segments of the lower lobe of the left lung. Chest. 1992; 102:1583–1585.14. Jiang S, Sun XW, Yu D, Jie B. Endovascular embolization of bronchial artery originating from the upper portion of aortic arch in patients with massive hemoptysis. Cardiovasc Intervent Radiol. 2014; 37:94–100.15. Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics. 2002; 22:1395–1409.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Bronchial Artery Arising from a Replaced Left Hepatic Artery in a Patient with Massive Hemoptysis
- A Case Report of Aberrant Bronchial Artery from Common Carotid Artery: A Potential Hazard in Bronchial Artery Embolization
- A Case of Pulmonary Artery-bronchial Fistula with Massive Hemoptysis due to Pulmonary Tuberculosis
- Bronchial artery embolization: clinical analysis of 129 cases
- A Case of Bilateral Intrapulmonary Sequestration
