Two Cases of Glomus Tumor Arising in Large Airway: Well Organized Radiologic, Macroscopic and Microscopic Findings
- Affiliations
-
- 1Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hanjho@skku.edu
- 2Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Abstract
- Glomus tumors of the lung are rare benign neoplasm, originating from modified smooth muscle cells. The patients are usually presented with no or non-specific symptoms such as cough, dyspnea or hemoptysis. Although surgical treatment is considered as the treatment of choice, the endobronchial therapy can be applied to the patients who are unfit for surgical excision. Herein, we describe two rare cases of glomus tumor originated at large airway (trachea and main bronchus) without respiratory symptoms and review their characteristic radiologic, macroscopic and pathological features.
Keyword
Figure
-
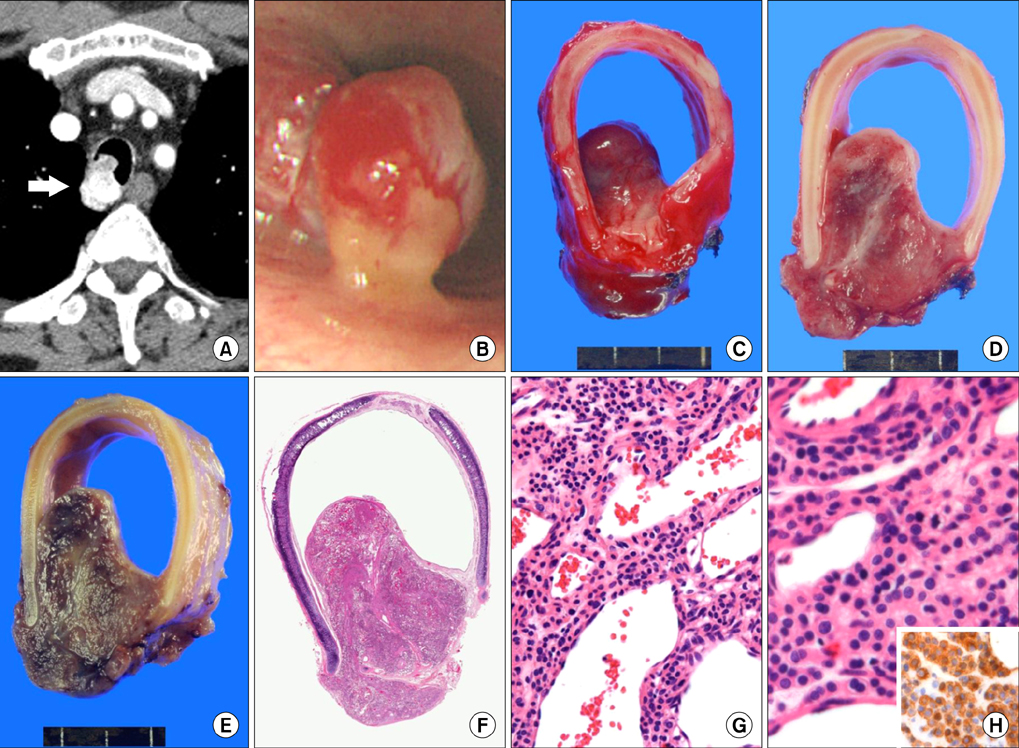
Figure 1 (A) Computed tomography reveals a highly enhanced 2.6 cm-sized, iceberg shaped tracheal tumor involving the right-side posterolateral. (B) Bronchoscopy reveals a 1 cm-sized mass with erythematous mucosal surface 7 cm below the vocal cord. (C) Grossly, the mass is internally protruded and has a reddish mucosal surface. (D) On section, it discloses a pinkish, meaty and solid cut surface without necrosis or hemorrhage. (E) After the fixation by formalin, the mass shows similar consistency and appearance with leiomyoma. (F) At low power view, the mass is well circumscribed and has abundant vasculature (H&E stain, 1:1 scan view). (G) It consists of proliferation of epithelioid cells showing perivascular arrangements with abundant vascular channels (H&E stain, ×200). (H) The tumor cells have abundant eosinophilic or clear cytoplasm and bland oval nuclei and shows positivity for smooth muscle actin (SMA) (H&E stain, ×400; inset: SMA, ×400).

Figure 2 (A) The 1.6 cm-sized highly enhanced nodule is noted in right main bronchus near carina. (B) Bronchoscopy reveals a sessile endobronchial mass with hyperemic surface near the carina. (C) Grossly, the mass is intraluminal polypoid growing and has flesh cut surface. (D) After the fixation by formalin, the mass shows gray solid cut surface with rubbery consistency. (E) At low power view, it is a well circumscribed, and ovoid mass. (F) The tumor cells consist of relatively uniformed epithelioid cells with bland-looking hyperchromatic nuclei and shows positivity for smooth muscle actin (inset) (F, ×400).
Reference
-
1. Shugart RR, Soule EH, Johnson EW Jr. Glomus Tumor. Surg Gynecol Obstet. 1963; 117:334–340.2. Miettinen M, Paal E, Lasota J, Sobin LH. Gastrointestinal glomus tumors: a clinicopathologic, immunohistochemical, and molecular genetic study of 32 cases. Am J Surg Pathol. 2002; 26:301–311.3. Albores-Saavedra J, Gilcrease M. Glomus tumor of the uterine cervix. Int J Gynecol Pathol. 1999; 18:69–72.4. Gokten N, Peterdy G, Philpott T, Maluf HM. Glomus tumor of the ovary: report of a case with immunohistochemical and ultrastructural observations. Int J Gynecol Pathol. 2001; 20:390–394.5. Kim MJ, Sung WJ. Primary pulmonary glomus tumor, diagnosed by preoperative needle biopsy: report of one case and literature review. Korean J Pathol. 2008; 42:37–40.6. Ariizumi Y, Koizumi H, Hoshikawa M, Shinmyo T, Ando K, Mochizuki A, et al. A primary pulmonary glomus tumor: a case report and review of the literature. Case Rep Pathol. 2012; 2012:782304.7. Lee EW, Kim SO, Oh IJ, Ju JY, Cho GJ, Kim KS, et al. A case of bronchial glomus tumor. Tuberc Respir Dis. 2002; 53:445–449.8. Jeffery PK. Remodeling in asthma and chronic obstructive lung disease. Am J Respir Crit Care Med. 2001; 164(10 Pt 2):S28–S38.9. Ko JM, Jung JI, Park SH, Lee KY, Chung MH, Ahn MI, et al. Benign tumors of the tracheobronchial tree: CT-pathologic correlation. AJR Am J Roentgenol. 2006; 186:1304–1313.10. Grillo HC, Mathisen DJ. Primary tracheal tumors: treatment and results. Ann Thorac Surg. 1990; 49:69–77.11. Akata S, Yoshimura M, Park J, Okada S, Maehara S, Usuda J, et al. Glomus tumor of the left main bronchus. Lung Cancer. 2008; 60:132–135.12. Glazebrook KN, Laundre BJ, Schiefer TK, Inwards CY. Imaging features of glomus tumors. Skeletal Radiol. 2011; 40:855–862.
