Tuberc Respir Dis.
2013 Dec;75(6):260-263.
Invasive Pulmonary Aspergillosis after Influenza A Infection in an Immunocompetent Patient
- Affiliations
-
- 1Department of Internal Medicine, Hallym University Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea.
- 2Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea.
- 3Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. p0702@chol.net
Abstract
- Invasive aspergillosis has emerged as a major cause of life-threatening infections in immunocompromised patients. Recently, patients with chronic obstructive pulmonary disease, who have been receiving corticosteroids for a long period, and immunocompetent patients in the intensive care unit have been identified as nontraditional hosts at risk for invasive aspergillosis. Here, we report a case of invasive pulmonary aspergillosis after influenza in an immunocompetent patient. The patient's symptoms were nonspecific, and the patient was unresponsive to treatments for pulmonary bacterial infection. Bronchoscopy revealed mucosa hyperemia, and wide, raised and cream-colored plaques throughout the trachea and both the main bronchi. Histologic examination revealed aspergillosis. The patient recovered quickly when treated systemically with voriconazole, although the reported mortality rates for aspergillosis are extremely high. This study showed that invasive aspergillosis should be considered in immunocompetent patients who are unresponsive to antibiotic treatments; further, early extensive use of all available diagnostic tools, especially bronchoscopy, is mandatory.
MeSH Terms
-
Adrenal Cortex Hormones
Aspergillosis
Bacterial Infections
Bronchi
Bronchoscopy
Humans
Hyperemia
Immunocompetence
Immunocompromised Host
Influenza A virus
Influenza, Human*
Intensive Care Units
Invasive Pulmonary Aspergillosis*
Mortality
Mucous Membrane
Pulmonary Disease, Chronic Obstructive
Trachea
Adrenal Cortex Hormones
Figure
-
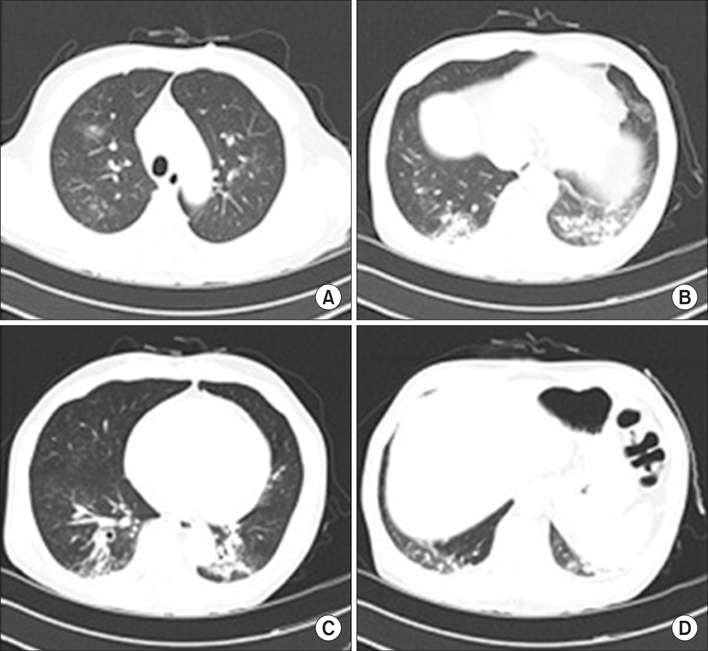
Figure 1 (A-D) Chest computed tomography findings. Multifocal ground glass opacities and peribronchial infiltration in both the lungs.
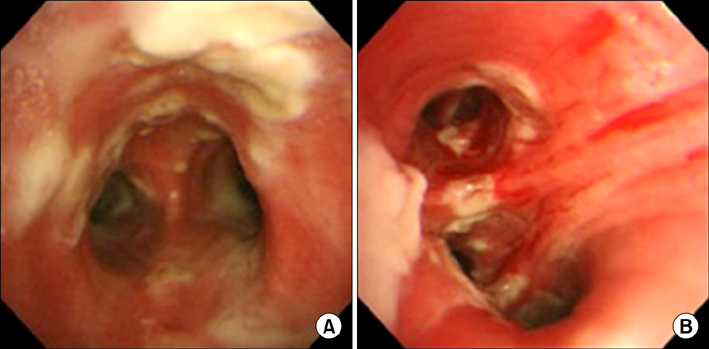
Figure 2 Bronchoscopic examination showing mucosa hyperemia and wide, raised and cream-colored plaques (pseudomembrane formation) through the carina (A) and the right bronchus intermedius (B).
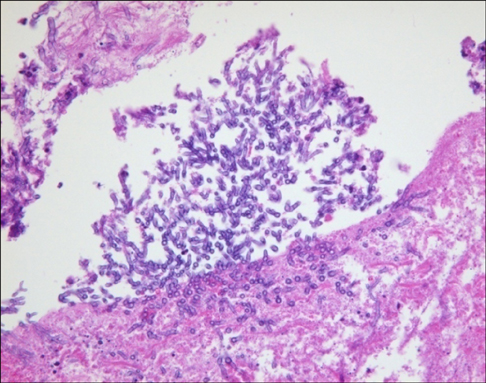
Figure 3 Histologic examination of bronchoscopic biopsy showing numerous branching septate hyphae (PAS stain, ×200).
Reference
-
1. Trof RJ, Beishuizen A, Debets-Ossenkopp YJ, Girbes AR, Groeneveld AB. Management of invasive pulmonary aspergillosis in non-neutropenic critically ill patients. Intensive Care Med. 2007; 33:1694–1703.2. Wauters J, Baar I, Meersseman P, Meersseman W, Dams K, De Paep R, et al. Invasive pulmonary aspergillosis is a frequent complication of critically ill H1N1 patients: a retrospective study. Intensive Care Med. 2012; 38:1761–1768.3. Lass-Flörl C, Roilides E, Loffler J, Wilflingseder D, Romani L. Minireview: host defence in invasive aspergillosis. Mycoses. 2013; 56:403–413.4. Xu XY, Sun HM, Zhao BL, Shi Y. Diagnosis of airway-invasive pulmonary aspergillosis by tree-in-bud sign in an immunocompetent patient: case report and literature review. J Mycol Med. 2013; 23:64–69.5. Lee HY, Kang HH, Kang JY, Kim SK, Lee SH, Chung YY, et al. A case of tracheobronchial aspergillosis resolved spontaneously in an immunocompetent host. Tuberc Respir Dis. 2012; 73:278–281.6. Greene RE, Schlamm HT, Oestmann JW, Stark P, Durand C, Lortholary O, et al. Imaging findings in acute invasive pulmonary aspergillosis: clinical significance of the halo sign. Clin Infect Dis. 2007; 44:373–379.7. Buchheidt D, Weiss A, Reiter S, Hartung G, Hehlmann R. Pseudomembranous tracheobronchial aspergillosis: a rare manifestation of invasive aspergillosis in a non-neutropenic patient with Hodgkin's disease. Mycoses. 2003; 46:51–55.8. Tasci S, Glasmacher A, Lentini S, Tschubel K, Ewig S, Molitor E, et al. Pseudomembranous and obstructive Aspergillus tracheobronchitis: optimal diagnostic strategy and outcome. Mycoses. 2006; 49:37–42.9. Lat A, Bhadelia N, Miko B, Furuya EY, Thompson GR 3rd. Invasive aspergillosis after pandemic (H1N1) 2009. Emerg Infect Dis. 2010; 16:971–973.10. Hasejima N, Yamato K, Takezawa S, Kobayashi H, Kadoyama C. Invasive pulmonary aspergillosis associated with influenza B. Respirology. 2005; 10:116–119.11. Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA, et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008; 46:327–360.12. De Rosa FG, Terragni P, Pasero D, Trompeo AC, Urbino R, Barbui A, et al. Combination antifungal treatment of pseudomembranous tracheobronchial invasive aspergillosis: a case report. Intensive Care Med. 2009; 35:1641–1643.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fatal Clinical Course of Probable Invasive Pulmonary Aspergillosis with Influenza B Infection in an Immunocompetent Patient
- Invasive Pulmonary Aspergillosis Invaded to Thoracic Vertebra in a Immunocompetent Host: A case report
- Concurrent Nocardia Related Brain Abscess and Semi-Invasive Pulmonary Aspergillosis in an Immunocompetent Patient
- Invasive Pulmonary Aspergillosis in a Immunocompetent Patient after Congenital Heart Disease Surgery: A Case Report
- A Case of Acute Cerebral Aspergillosis Complicating Influenza A/H1N1pdm 2009
