Combined Intrathoracic and Intraperitoneal Splenosis after Splenic Injury: Case Report and Review of the Literature
- Affiliations
-
- 1Division of Pulmonology, Department of Internal Medicine, Institute of Chest Disease, Seoul, Korea. STOPYES@yuhs.ac
- 2Department of Nuclear Medicine, Yonsei University College of Medicine, Seoul, Korea.
Abstract
- Splenosis is defined as an autotransplantation of the splenic tissue after splenic rupture or splenectomy, and occurs most frequently in the peritoneal cavity. Splenosis is usually asymptomatic and is found incidentally. We report a case of combined intrathoracic and intraperitoneal splenosis in a 54-year-old male who worked as a miner for 10 years in his twenties, and was a current smoker. He was referred to our hospital for further evaluation of an incidental left diaphragmatic mass. Positron emission tomography-computed tomography and bronchoscopy were performed to evaluate the possibility of malignancy. There was no evidence of malignancy, but the spleen was not visualized. Reviewing his medical history revealed previous splenectomy, following a dynamite explosion injury. Therefore, splenosis was suspected and technetium-99m-labeled heat-damaged red blood cell scan confirmed the diagnosis. Radionuclide imaging is a useful diagnostic tool for splenosis, which could avoid unnecessary invasive procedures.
Keyword
MeSH Terms
Figure
-
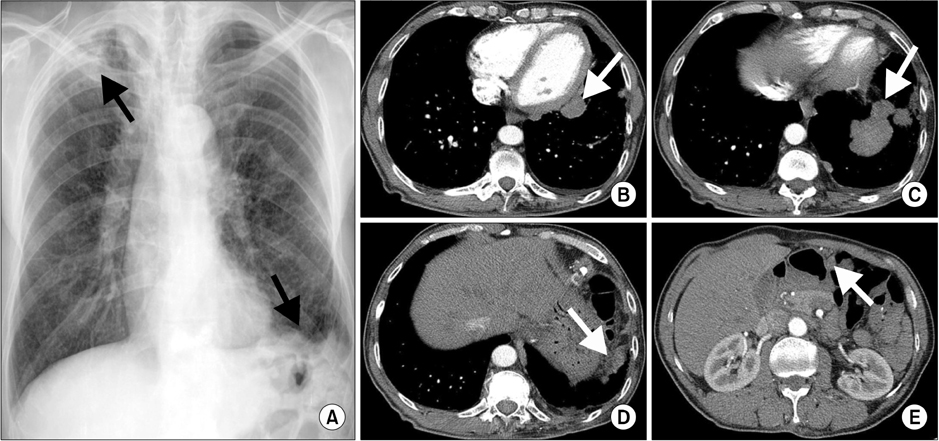
Figure 1 (A) Chest X-ray showing a left diaphragmatic mass with irregular margin and consolidation in the right upper lobe. (B-E) Chest computed tomography. Multiple lobulated masses and nodules present along the left lower mediastinum (B), left diaphragm (C, D), and omentum (E).
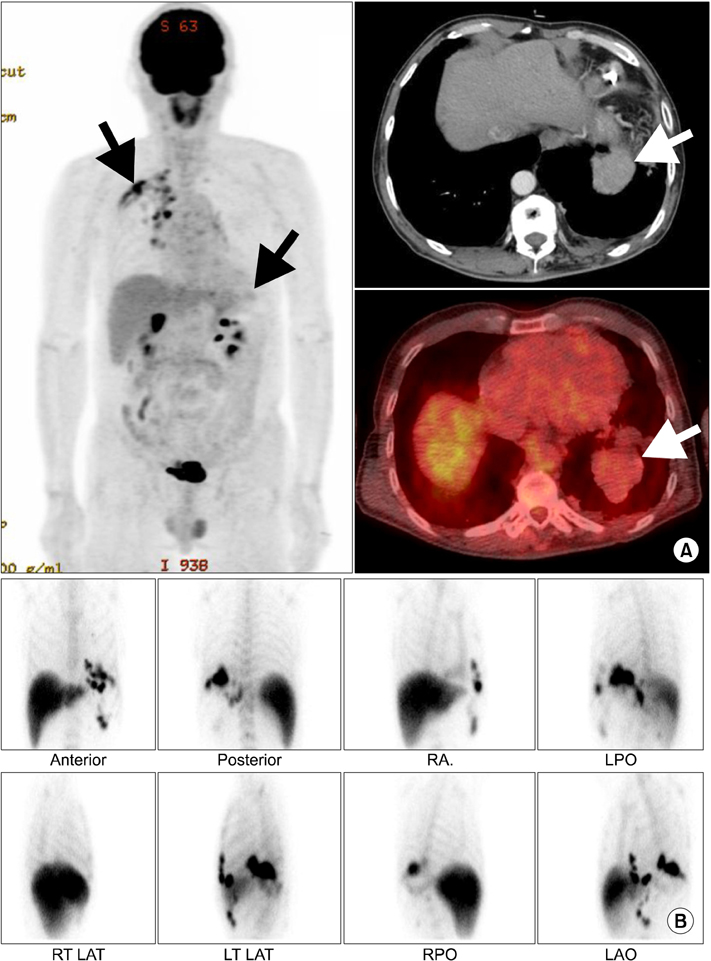
Figure 2 (A) Positron emission tomography computed tomography (PET-CT). Multiple masses and nodules along left diaphragm and multiple small nodular lesions in the left perigastric area and omentum show faint fluoro-2-deoxygluocose (FDG) uptake. Moreover, acute and chronic inflammation with fibrosis and calcified granulomas were observed in the right upper lobe with intense FDG uptake. (B) Technetium-99m-labeled heat-damaged red blood cell scan. Multiple foci show increased uptake in the left thorax and left upper quadrant of the abdomen, consistent with thoracic and abdominal splenosis. RAO: right anterior oblique; LPO: left posterior oblique; RT LAT: right lateral; LT LAT: left lateral; RPO: right posterior oblique; LAO: left anterior oblique.
Reference
-
1. Hoh JK, Kim KT, Cho SH, Hwang YY. A case of pelvic splenosis after splenectomy: a cause of pelvic pain. Korean J Obstet Gynecol. 2005. 48:3004–3008.2. Kim KA, Park CM, Kim CH, Choi SY, Park SW, Kang EY, et al. An interesting hepatic mass: splenosis mimicking a hepatocellular carcinoma (2003:9b). Eur Radiol. 2003. 13:2713–2715.3. Ryu SW, Kim IH, Sohn SS. Splenosis mimicking carcinomatosis peritonei in advanced gastric cancer. J Korean Surg Soc. 2005. 68:61–64.4. Yoon M, Hwang KH, Choe W. Multifocal peritoneal splenosis in Tc-99m-labeled heat-denatured red blood cell scintigraphy. Nucl Med Mol Imaging. 2006. 40:190–191.5. Choi GH, Ju MK, Kim JY, Kang CM, Kim KS, Choi JS, et al. Hepatic splenosis preoperatively diagnosed as hepatocellular carcinoma in a patient with chronic hepatitis B: a case report. J Korean Med Sci. 2008. 23:336–341.6. Bang SY, Paik CH, Chung YW, Chang MH, Kim JE, Kim YS, et al. A case of intraperitoneal splenosis: clinical history and imaging features avoided the need for invasive diagnostic procedures. Korean J Med. 2008. 74:Suppl 1. S33–S36.7. Chung SJ, Jahng JH, Mun HS, Park YA, Jung WH, Yu JS, et al. Case of colonic polyps with abdominal splenosis mimicking carcinomatosis. Korean J Med. 2008. 75:574–576.8. Kim K, Choi HJ, Kim YM, Kwon WJ, Lee WC, Suh JH. Thoracic splenosis: a case report and the importance of clinical history. J Korean Med Sci. 2010. 25:299–303.9. Kang KC, Cho GS, Chung GA, Kang GH, Kim YJ, Lee MS, et al. Intrahepatic splenosis mimicking liver metastasis in a patient with gastric cancer. J Gastric Cancer. 2011. 11:64–68.10. von Kuttner H. In diskussion, milzextirpation und rontgenbehandlung bei leukamie. Berl Klin Wochenschr. 1910. 47:1520.11. Bernard Shaw AF, Shafi A. Traumatic autoplastic transplantation of splenic tissue in man with observations on the late results of splenectomy in six cases. J Pathol Bacteriol. 1937. 45:215–235.12. Kwok CM, Chen YT, Lin HT, Su CH, Liu YS, Chiu YC. Portal vein entrance of splenic erythrocytic progenitor cells and local hypoxia of liver, two events cause intrahepatic splenosis. Med Hypotheses. 2006. 67:1330–1332.13. Fremont RD, Rice TW. Splenosis: a review. South Med J. 2007. 100:589–593.14. Cordier JF, Gamondes JP, Marx P, Heinen I, Loire R. Thoracic splenosis presenting with hemoptysis. Chest. 1992. 102:626–627.15. Armas RR. Clinical studies with spleen-specific radiolabeled agents. Semin Nucl Med. 1985. 15:260–275.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intrahepatic Splenosis Mimicking Hepatocellular Carcinoma: A Case Report
- Two Rare Cases of Intrathoracic Splenosis and Subcutaneous Splenosis: Spleen Scintigraphy Avoided the Need for Invasive Procedures
- Splenosis with Cyclic Abdominal Pain Misdiagnosed as Ovarian Dermoid Cyst
- Thoracic Splenosis after Splenic and Diaphragmatic Injury
- Thoracic Splenosis: A Case Report and Noninvasive Diagnosis
