Sarcoidosis Induced by Adalimumab in Rheumatoid Arthritis
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. whitedawne@hanmail.net
Abstract
- Adalimumab is a full human monoclonal antibody that inhibits tumor necrosis factor-alpha (TNF-alpha). This has recently been shown to be effective in the treatment of rheumatoid arthritis (RA), ankylosing spondylitis, and other conditions. Sacoidosis is known to be the target for adalimumab but we describe a patient who has developed sarcoidosis with lung involvement during adalimumab therapy for RA. A 48-year-old woman, who was treated with adalimumab for 5 months, was admitted because of chronic cough and both hilar lymphadenopathy on chest radiography. Chest computed tomography revealed the enlargement of multiple lymph nodes in the right supraclavicular, subcarinal, both hilar and right axillary area. She was diagnosed with sarcoidosis based on the biopsy of supraclavicular lymph node, skin and lung through video-associated thoracoscopic surgery, which was non-caseating epitheloid cell granuloma and excluded from a similar disease. She was treated for sarcoidosis with prednisolone and methotrexate instead of adalimumab.
Keyword
MeSH Terms
-
Antibodies, Monoclonal, Humanized
Arthritis, Rheumatoid
Biopsy
Cough
Female
Granuloma
Humans
Lung
Lymph Nodes
Lymphatic Diseases
Methotrexate
Middle Aged
Prednisolone
Sarcoidosis
Skin
Spondylitis, Ankylosing
Thoracoscopy
Thorax
Tumor Necrosis Factor-alpha
Adalimumab
Antibodies, Monoclonal, Humanized
Methotrexate
Prednisolone
Tumor Necrosis Factor-alpha
Figure
-
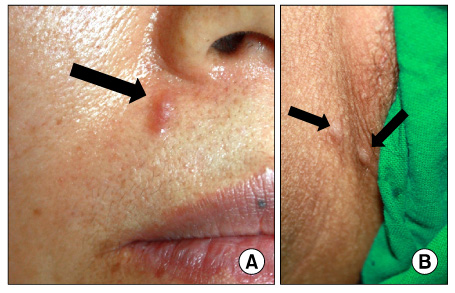
Figure 1 Photography of skin lesions. Face (A) and inguinal area (B). There were localized erythematous papules (arrow).
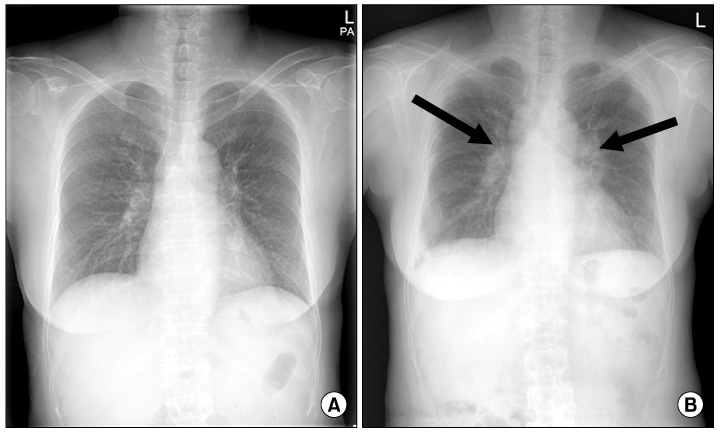
Figure 2 Simple chest radiography. Chest X-ray shows normal findings 6 months earlier (A) and both hilar lymph node (arrows) enlargement at a regular follow-up (B).
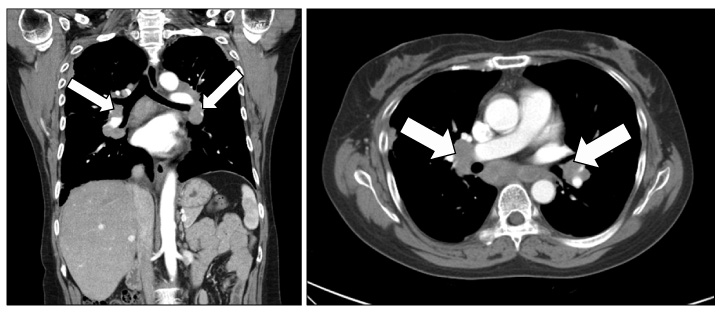
Figure 3 Chest CT scans show both hilar, subcarinal lymphadenopathy and right upper paratracheal lymphadenopathy (arrow). CT: computed tomography.
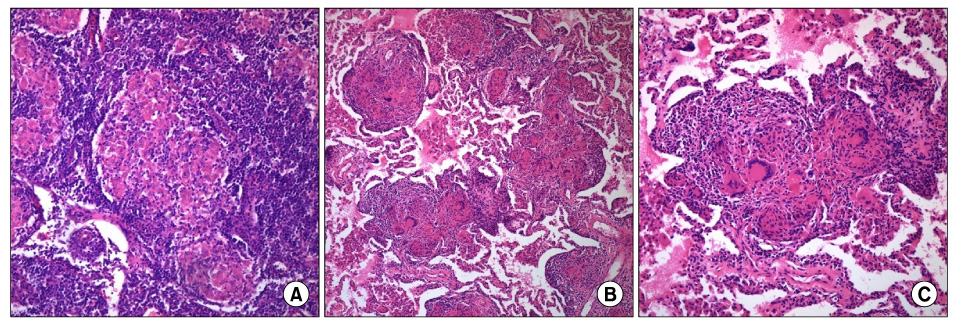
Figure 4 Supraclavicular lymph node and lung biopsy showing evenly distributed small non caseating granulomas (A) Supraclavicular lymph node biopsy (H&E stain ×200). (B) Lung biopsy (H&E stain ×100). (C) Lung biopsy (H&E stain ×200).

Figure 5 Simple chest radiography after treatment with systemic corticosteroid and MTX. Chest X-ray shows improvement in the hilar lymphadenopathy and peripheral infiltrates.
Reference
-
1. Tak PP, Kalden JR. Advances in rheumatology: new targeted therapeutics. Arthritis Res Ther. 2011. 13:Suppl 1. S5.2. Senolt L, Vencovský J, Pavelka K, Ospelt C, Gay S. Prospective new biological therapies for rheumatoid arthritis. Autoimmun Rev. 2009. 9:102–107.3. Lahmer T, Knopf A, Lanzl I, Heemann U, Thuermel K. Using TNF-alpha antagonist Adalimumab for treatment for multisystem sarcoidosis: a case study. Rheumatol Int. 2011. 06. 05. [Epub]. DOI: 10.1007/s00296-011-1968-x.4. Javot L, Tala S, Scala-Bertola J, Massy N, Trenque T, Baldin B, et al. Sarcoïdosis and anti-TNF: a paradoxical class effect? Analysis of the French pharmacovigilance system database and literature review. Therapie. 2011. 66:149–154.5. Toussirot E, Pertuiset E, Kantelip B, Wendling D. Sarcoidosis occuring during anti-TNF-alpha treatment for inflammatory rheumatic diseases: report of two cases. Clin Exp Rheumatol. 2008. 26:471–475.6. Clementine RR, Lyman J, Zakem J, Mallepalli J, Lindsey S, Quinet R. Tumor necrosis factor-alpha antagonist-induced sarcoidosis. J Clin Rheumatol. 2010. 16:274–279.7. Murdaca G, Colombo BM, Puppo F. Adalimumab for the treatment of immune-mediated diseases: an update on old and recent indications. Drugs Today (Barc). 2011. 47:277–288.8. Pink AE, Fonia A, Smith CH, Barker JN. The development of sarcoidosis on antitumour necrosis factor therapy: a paradox. Br J Dermatol. 2010. 163:648–649.9. Ramos-Casals M, Roberto-Perez-Alvarez , Diaz-Lagares C, Cuadrado MJ, Khamashta MA. BIOGEAS Study Group. Autoimmune diseases induced by biological agents: a double-edged sword? Autoimmun Rev. 2010. 9:188–193.10. Kerjouan M, Jouneau S, Lena H, Luraine R, Desrues B, Delaval P. Pulmonary sarcoidosis developing during treatment with etanercept. Rev Mal Respir. 2011. 28:360–364.11. Gifre L, Ruiz-Esquide V, Xaubet A, Gómez-Puerta JA, Hernández MV, Sanmartí R. Lung sarcoidosis induced by TNF antagonists in rheumatoid arthritis: a case presentation and a literature review. Arch Bronconeumol. 2011. 47:208–212.12. Toussirot E, Pertuiset E, Kantelip B, Wendling D. Sarcoidosis occuring during anti-TNF-alpha treatment for inflammatory rheumatic diseases: report of two cases. Clin Exp Rheumatol. 2008. 26:471–475.13. Daïen CI, Monnier A, Claudepierre P, Constantin A, Eschard JP, Houvenagel E, et al. Sarcoid-like granulomatosis in patients treated with tumor necrosis factor blockers: 10 cases. Rheumatology (Oxford). 2009. 48:883–886.14. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007. 357:2153–2165.15. Furst DE, Wallis R, Broder M, Beenhouwer DO. Tumor necrosis factor antagonists: different kinetics and/or mechanisms of action may explain differences in the risk for developing granulomatous infection. Semin Arthritis Rheum. 2006. 36:159–167.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Development of Rheumatoid Nodules after Anti-Tumor Necrosis Factor-α Treatment with Adalimumab for Rheumatoid Arthritis
- New-onset Psoriasis Induced by Adalimumab Administered for Rheumatoid Arthritis
- Adalimumab-induced Lupus Erythematosus Profundus in a Rheumatoid Arthritis Patient
- A Case of Early Onset Sarcoidosis Masquerading as Juvenile Rheumatoid Arthritis
- Adalimumab Induced Acute Exacerbation of Rheumatoid Arthritis Related Interstitial Lung Disease
