A Case of Tuberculous Pericardial Abscess Mimicking Thymic Carcinoma
- Affiliations
-
- 1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea. f2000tj@naver.com
- 2Department of Thoracic and Cardiovascular Surgery, Hallym University Sacred Heart Hospital, Anyang, Korea.
- 3Department of Pathology, Hallym University Sacred Heart Hospital, Anyang, Korea.
Abstract
- We report here an unusual case of pericardial tuberculoma that was misdiagnosed as thymic carcinoma on an imaging study. A 48-year-old woman was referred for evaluation of an anterior mediastinal mass. Computed tomography (CT) scans of the chest displayed cystic masses mimicking thymic carcinoma at the anterior mediastinum. Pericardiotomy and surgical drainage of the cystic masses were done, and pathologic examination of the excised pericardial specimen showed a chronic granulomatous inflammation with necrosis, compatible with tuberculosis. Acid-fast bacilli were also identified in the specimen. After treatment with anti-tuberculosis drugs and steroids, the patient showed clinical improvement. Although tuberculous pericarditis usually presents as pericardial effusion or constrictive pericarditis, it can also present as a pericardial mass mimicking thymic carcinoma on CT. Therefore, we suggest that tuberculous pericardial abscess should be included in the differential diagnosis of a mediastinal mass in Korea, with intermediate tuberculosis prevalence.
Keyword
MeSH Terms
Figure
-
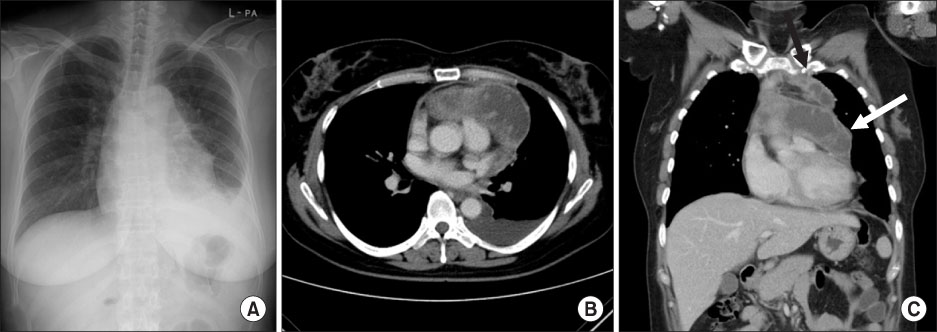
Figure 1 (A) Chest PA on admission shows anterior mediastinal widening with left pleural effusion. (B, C) Initial chest CT scans with transverse and coronal images. Chest CT scan displays multi-loculated two cystic masses at the anterior mediastinum (white arrow, 10.5×4.2 cm; black arrow, 6.8×1.7 cm) with peripheral enhancement. No foci of calcification were observed within the mass. PA: Posterior anterior; CT: computed tomography.

Figure 2 PET/CT images show FDG uptake in the pericardial lesion with a maximal SUV of 8.3 and central photon defect area. PET: positron emission tomography; CT: computed tomography; FDG: fludeoxyglucose; SUV: standardized uptake value.
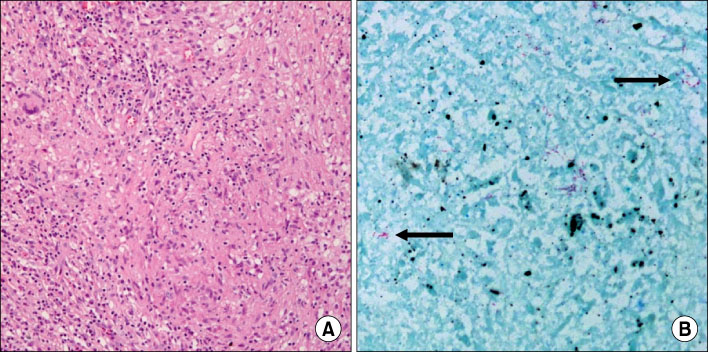
Figure 3 (A) Pathologic examination of the excised pericardial specimen shows a chronic granulomatous inflammation with necrosis, compatible with tuberculosis (H&E stain, ×100). (B) Acid-fast bacillus was also indentified (black arrow, AFB stain, ×200).
Reference
-
1. Golden MP, Vikram HR. Extrapulmonary tuberculosis: an overview. Am Fam Physician. 2005. 72:1761–1768.2. Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005. 112:3608–3616.3. Zayas R, Anguita M, Torres F, Giménez D, Bergillos F, Ruiz M, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995. 75:378–382.4. Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest. 2005. 128:2893–2909.5. Korea Centers for Disease Control & Prevention. Annual report on the notified tuberculosis patients in Korea 2009. 2010. Seoul: Korea Centers for Disease Control & Prevention.6. Wang ZJ, Reddy GP, Gotway MB, Yeh BM, Hetts SW, Higgins CB. CT and MR imaging of pericardial disease. Radiographics. 2003. 23:S167–S180.7. Lin TH, Chiu CC, Huang CH, Tsai KB, Sheu SH. Tuberculous pericardial abscess: a case report. Kaohsiung J Med Sci. 2005. 21:322–325.8. Agrawal S, Radhakrishnan S, Sinha N. Echocardiographic demonstration of resolving intrapericardial mass in tuberculous pericardial effusion. Int J Cardiol. 1990. 26:240–241.9. Kim JH, Yoo JH, Choi CY, Woo TW, Kim NH, Kim YH, et al. A giant cystic mediastinal tuberculosis communicating with pericardium. Tuberc Respir Dis. 2002. 53:439–444.10. Hegde AN, Desai SB, Shivdasani B. Tuberculous pericardial abscess. Eur J Cardiothorac Surg. 2005. 28:166.11. Fowler NO. Tuberculous pericarditis. JAMA. 1991. 266:99–103.12. Sadohara J, Fujimoto K, Müller NL, Kato S, Takamori S, Ohkuma K, et al. Thymic epithelial tumors: comparison of CT and MR imaging findings of low-risk thymomas, high-risk thymomas, and thymic carcinomas. Eur J Radiol. 2006. 60:70–79.13. Wang YT, Lu F, Zhu F, Qian ZB, Xu YP, Meng T. Primary hepatic tuberculoma appears similar to hepatic malignancy on F-18 FDG PET/CT. Clin Nucl Med. 2009. 34:528–529.14. Chang JM, Lee HJ, Goo JM, Lee HY, Lee JJ, Chung JK, et al. False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol. 2006. 7:57–69.
