Tuberc Respir Dis.
2010 Sep;69(3):184-190.
Chest CT Parameters to Predict the Major Adverse Events in Acute Submassive Pulmonary Embolism
- Affiliations
-
- 1Department of Emergency Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. wonpia@yahoo.co.kr
- 2Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Respiratory and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Abstract
- BACKGROUND
The purpose of this study was to determine the prognostic significance of chest computed tomographic (CT) parameters in acute submassive pulmonary embolism (PE).
METHODS
Between January 2006 and December 2009, 268 consecutive patients with acute submassive PE that was confirmed by chest CT with pulmonary angiography in emergency room were studied. One experienced radiologist measured CT parameters and judged the presence of right ventricular dysfunction. CT parameters were analyzed to determine their ability to predict a major adverse event (MAE).
RESULTS
There were 220 patients included and 61 (27.7%) had MAE. Left ventricular and right ventricular maximum minor axis (36.4+/-8.0 vs. 41.7+/-7.4, p<0.01; 45.7+/-9.4 vs. 41.5+/-7.6, p<0.01), superior vena cava diameter (19.2+/-3.4 vs. 18.0+/-3.4, p=0.02), azygos vein diameter (10.0+/-2.2 vs. 9.2+/-2.3, p=0.02), septal displacement (19 vs. 18, p<0.01) were significantly higher in MAE group than in no MAE group. Patients with MAE had high right ventricular/left ventricular dimension ratio (RV/LV ratio) compared to patients without MAE (1.34+/-0.48 vs. 1.03+/-0.28, p<0.01). The most useful cut-off value of RV/LV ratio for MAE was 1.3 and the area under the curve was 0.71 (0.62~0.79).
CONCLUSION
RV/LV ratio on chest CT was a significant predictor of submassive PE related shock, intubation, in-hospital mortality, thrombolysis, thrombectomy within 30 days.
Keyword
MeSH Terms
Figure
-
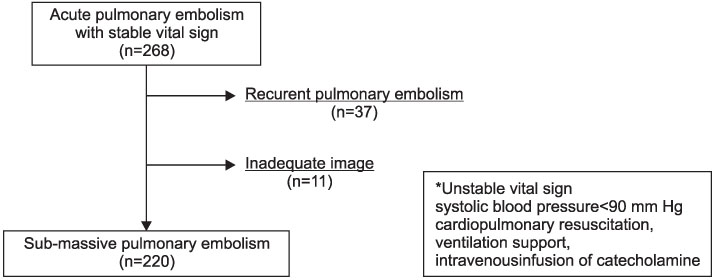
Figure 1 Selection of patients.

Figure 2 Receiver operating characteristic curve for predicting major adverse events with RV/LV dimension ratio on 16 slice multidetector scanner.
Reference
-
1. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999. 353:1386–1389.2. Scientific Committee for National Survey of Acute Pulmonary Thromboembolism, Korean Academy of Tuberculosis and Respiratory Diseases. The national survey of acute pulmonary thromboembolism in Korea. Tuberc Respir Dis. 2003. 54:5–14.3. Kucher N, Wallmann D, Carone A, Windecker S, Meier B, Hess OM. Incremental prognostic value of troponin I and echocardiography in patients with acute pulmonary embolism. Eur Heart J. 2003. 24:1651–1656.4. La Vecchia L, Ottani F, Favero L, Spadaro GL, Rubboli A, Boanno C, et al. Increased cardiac troponin I on admission predicts in-hospital mortality in acute pulmonary embolism. Heart. 2004. 90:633–637.5. Kostrubiec M, Pruszczyk P, Bochowicz A, Pacho R, Szulc M, Kaczynska A, et al. Biomarker-based risk assessment model in acute pulmonary embolism. Eur Heart J. 2005. 26:2166–2172.6. van der Meer RW, Pattynama PM, van Strijen MJ, van den Berg-Huijsmans AA, Hartmann IJ, Putter H, et al. Right ventricular dysfunction and pulmonary obstruction index at helical CT: prediction of clinical outcome during 3-month follow-up in patients with acute pulmonary embolism. Radiology. 2005. 235:798–803.7. Ribeiro A, Lindmarker P, Juhlin-Dannfelt A, Johnsson H, Jorfeldt L. Echocardiography Doppler in pulmonary embolism: right ventricular dysfunction as a predictor of mortality rate. Am Heart J. 1997. 134:479–487.8. Kasper W, Konstantinides S, Geibel A, Tiede N, Krause T, Just H. Prognostic significance of right ventricular afterload stress detected by echocardiography in patients with clinically suspected pulmonary embolism. Heart. 1997. 77:346–349.9. Burgess MI, Bright-Thomas RJ, Ray SG. Echocardiographic evaluation of right ventricular function. Eur J Echocardiogr. 2002. 3:252–262.10. Ghaye B, Remy J, Remy-Jardin M. Non-traumatic thoracic emergencies: CT diagnosis of acute pulmonary embolism: the first 10 years. Eur Radiol. 2002. 12:1886–1905.11. He H, Stein MW, Zalta B, Haramati LB. Computed tomography evaluation of right heart dysfunction in patients with acute pulmonary embolism. J Comput Assist Tomogr. 2006. 30:262–266.12. Ghuysen A, Ghaye B, Willems V, Lambermont B, Gerard P, Dondelinger RF, et al. Computed tomographic pulmonary angiography and prognostic significance in patients with acute pulmonary embolism. Thorax. 2005. 60:956–961.13. Task Force on Pulmonary Embolism, European Society of Cardiology. Guidelines on diagnosis and management of acute pulmonary embolism. Eur Heart J. 2000. 21:1301–1336.14. Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galiè N, Pruszczyk P, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008. 29:2276–2315.15. Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, et al. Short-term clinical outcome of patients with acute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation. 2000. 101:2817–2822.16. Kucher N, Rossi E, De Rosa M, Goldhaber SZ. Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med. 2005. 165:1777–1781.17. Quiroz R, Kucher N, Schoepf UJ, Kipfmueller F, Solomon SD, Costello P, et al. Right ventricular enlargement on chest computed tomography: prognostic role in acute pulmonary embolism. Circulation. 2004. 109:2401–2404.18. Collomb D, Paramelle PJ, Calaque O, Bosson JL, Vanzetto G, Barnoud D, et al. Severity assessment of acute pulmonary embolism: evaluation using helical CT. Eur Radiol. 2003. 13:1508–1514.19. Schoepf UJ, Kucher N, Kipfmueller F, Quiroz R, Costello P, Goldhaber SZ. Right ventricular enlargement on chest computed tomography: a predictor of early death in acute pulmonary embolism. Circulation. 2004. 110:3276–3280.20. Contractor S, Maldjian PD, Sharma VK, Gor DM. Role of helical CT in detecting right ventricular dysfunction secondary to acute pulmonary embolism. J Comput Assist Tomogr. 2002. 26:587–591.21. Jardin F, Dubourg O, Bourdarias JP. Echocardiographic pattern of acute cor pulmonale. Chest. 1997. 111:209–217.22. Qanadli SD, El Hajjam M, Vieillard-Baron A, Joseph T, Mesurolle B, Oliva VL, et al. New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol. 2001. 176:1415–1420.23. Wu AS, Pezzullo JA, Cronan JJ, Hou DD, Mayo-Smith WW. CT pulmonary angiography: quantification of pulmonary embolus as a predictor of patient outcome--initial experience. Radiology. 2004. 230:831–835.24. Araoz PA, Gotway MB, Trowbridge RL, Bailey RA, Auerbach AD, Reddy GP, et al. Helical CT pulmonary angiography predictors of in-hospital morbidity and mortality in patients with acute pulmonary embolism. J Thorac Imaging. 2003. 18:207–216.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Outcome Related to Diagnosis of Saddle Pulmonary Embolism using Computed Tomographic Angiography in an Emergency Department
- Short-Term Mortality in Patients with Massive and Submassive Pulmonary Embolism Receiving Thrombolytic Therapy
- The Ratio of Descending Aortic Enhancement to Main Pulmonary Artery Enhancement Measured on Pulmonary CT Angiography as a Finding to Predict Poor Outcome in Patients with Massive or Submassive Pulmonary Embolism
- Thrombolysis in Pulmonary Embolism
- Acute Right Intracardiac Thrombus-in-Transit Complicated by Submassive Pulmonary Embolism
