The Ratio of Descending Aortic Enhancement to Main Pulmonary Artery Enhancement Measured on Pulmonary CT Angiography as a Finding to Predict Poor Outcome in Patients with Massive or Submassive Pulmonary Embolism
- Affiliations
-
- 1Department of Diagnostic Radiology, Bundang CHA Hospital, CHA University School of Medicine, Seongnam, Korea. smyoo68@hanmail.net
- 2Department of Preventive Medicine, CHA University School of Medicine, Pocheon, Korea.
- 3Department of Diagnostic Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
Abstract
- BACKGROUND
The purpose of this study was to evaluate whether measuring the ratio of descending aortic enhancement (DAE) to main pulmonary artery enhancement (MPAE) on pulmonary computed tomography angiography (PCTA) can predict poor outcome in patients with acute massive or submassive pulmonary embolism (PE).
METHODS
We retrospectively, reviewed computed tomgraphy findings and charts of 37 patients with acute PE and right ventricular dysfunction. We divided the enrolled patients into 3 groups; group Ia (n=8), comprised of patients with major adverse event (MAE); group Ib (n=5), consisted of those with PE-related MAE; and group II (n=29), those without MAE. We analyzed the right ventricular diameter (RVD)/left ventricular diameter (LVD) and DAE/MPAE on PCTA.
RESULTS
For observer 1, RVD/LVD in group Ia (1.9+/-0.36 vs. 1.44+/-0.38, p=0.009) and group Ib (1.87+/-0.37 vs. 1.44+/-0.38, p=0.044) were significantly higher than that of group II. For observer 2, RVD/LVD in group Ia (1.71+/-0.18 vs. 1.41+/-0.47, p=0.027) was significantly greater than that of group II, but RVD/LVD of group Ib was not (1.68+/-0.2 vs. 1.41+/-0.47, p=0.093). For both observers, there was a significant difference of DAE/MPAE between group Ib and group II (0.32+/-0.15 vs. 0.64+/-0.24, p=0.005; 0.34+/-0.16 vs. 0.64+/-0.22, p=0.004), but no significant difference of DAE/MPAE between group Ia and group II (0.51+/-0.3 vs. 0.64+/-0.24, p=0.268; 0.53+/-0.29 vs. 0.64+/-0.22, p=0.302). Intra-class correlation coefficient (ICC) for the measurement of DAE/MPAE (ICC=0.97) was higher than that of RVD/LVD (ICC=0.74).
CONCLUSION
DAE/MPAE measured on PCTA may predict PE-related poor outcomes in patients with massive or submassive PE with an excellent inter-observer agreement.
MeSH Terms
Figure
-
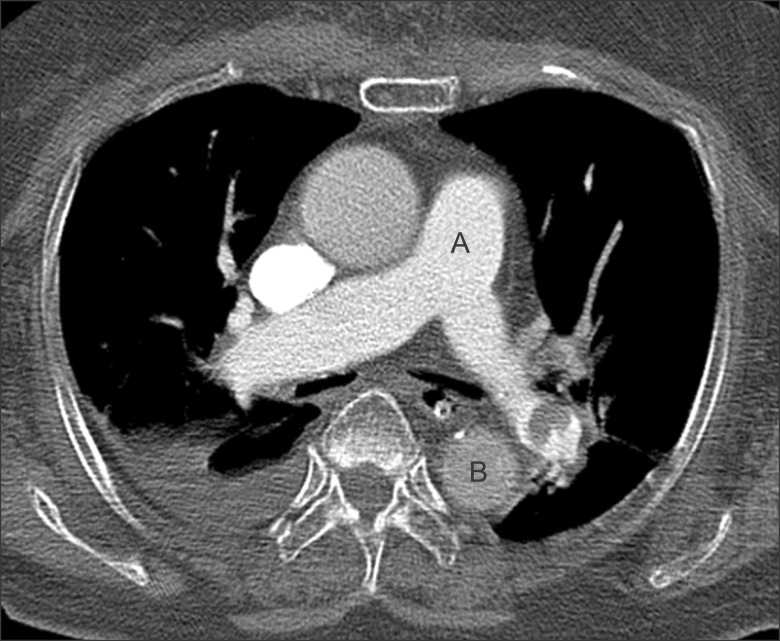
Figure 1 An example measuring the ratio of the descending aorta enhancement to the main pulmonary artery enhancement. Enhancement of the main pulmonary artery is measured at the level of bifurcation point of both main pulmonary arteries (A). Enhancement of the descending aorta is measured at the same level (B). Region of interest cursor is carefully placed to avoid beam hardening artifact caused by contrast material in the superior vena cava.
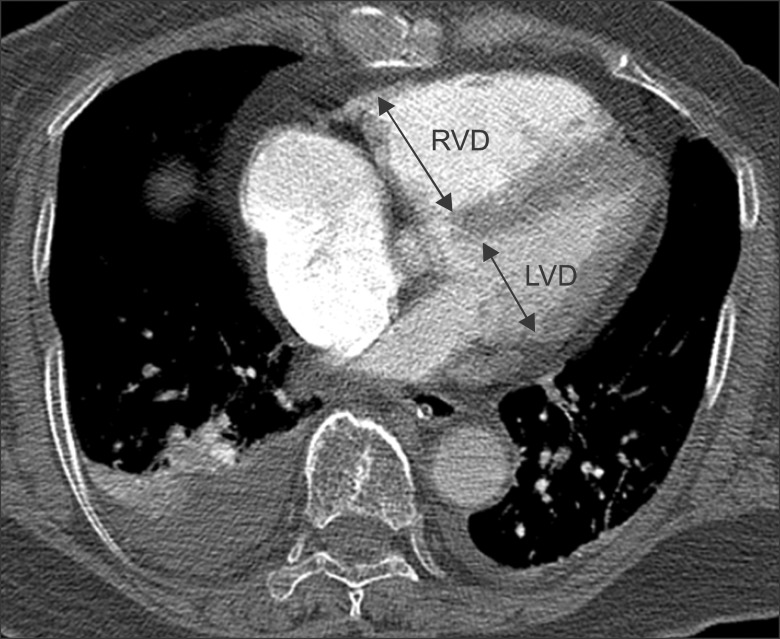
Figure 2 An example measuring the ratio of the right ventricular diameter to the left ventricular diameter. Diameter of the right and left ventricle is measured perpendicular to the long axis of the heart at a plane which has the largest diameter from one endocardial margin to the other. RVD: right ventricle diameter; LVD: left ventricle diameter.
Reference
-
1. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999; 353:1386–1389. PMID: 10227218.
Article2. Sanchez O, Trinquart L, Colombet I, Durieux P, Huisman MV, Chatellier G, et al. Prognostic value of right ventricular dysfunction in patients with haemodynamically stable pulmonary embolism: a systematic review. Eur Heart J. 2008; 29:1569–1577. PMID: 18495689.
Article3. Kucher N, Rossi E, De Rosa M, Goldhaber SZ. Massive pulmonary embolism. Circulation. 2006; 113:577–582. PMID: 16432055.
Article4. Kasper W, Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser KD, et al. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J Am Coll Cardiol. 1997; 30:1165–1171. PMID: 9350909.
Article5. Piazza G, Goldhaber SZ. Management of submassive pulmonary embolism. Circulation. 2010; 122:1124–1129. PMID: 20837937.
Article6. Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galiè N, Pruszczyk P, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008; 29:2276–2315. PMID: 18757870.7. Schoepf UJ, Kucher N, Kipfmueller F, Quiroz R, Costello P, Goldhaber SZ. Right ventricular enlargement on chest computed tomography: a predictor of early death in acute pulmonary embolism. Circulation. 2004; 110:3276–3280. PMID: 15533868.8. Collomb D, Paramelle PJ, Calaque O, Bosson JL, Vanzetto G, Barnoud D, et al. Severity assessment of acute pulmonary embolism: evaluation using helical CT. Eur Radiol. 2003; 13:1508–1514. PMID: 12835961.
Article9. Ghaye B, Ghuysen A, Willems V, Lambermont B, Gerard P, D'Orio V, et al. Severe pulmonary embolism: pulmonary artery clot load scores and cardiovascular parameters as predictors of mortality. Radiology. 2006; 239:884–891. PMID: 16603659.10. van der Meer RW, Pattynama PM, van Strijen MJ, van den Berg-Huijsmans AA, Hartmann IJ, Putter H, et al. Right ventricular dysfunction and pulmonary obstruction index at helical CT: prediction of clinical outcome during 3-month follow-up in patients with acute pulmonary embolism. Radiology. 2005; 235:798–803. PMID: 15845793.
Article11. Kang DK, Sun JS, Park KJ, Lim HS. Usefulness of combined assessment with computed tomographic signs of right ventricular dysfunction and cardiac troponin T for risk stratification of acute pulmonary embolism. Am J Cardiol. 2011; 108:133–140. PMID: 21529730.
Article12. Jung SK, Kim WY, Lee CW, Seo DW, Lee YS, Lee JH, et al. Chest CT parameters to predict the major adverse events in acute submassive pulmonary embolism. Tuberc Respir Dis. 2010; 69:184–190.
Article13. Araoz PA, Gotway MB, Harrington JR, Harmsen WS, Mandrekar JN. Pulmonary embolism: prognostic CT findings. Radiology. 2007; 242:889–897. PMID: 17325073.
Article14. Ghaye B, Ghuysen A, Bruyere PJ, D'Orio V, Dondelinger RF. Can CT pulmonary angiography allow assessment of severity and prognosis in patients presenting with pulmonary embolism? What the radiologist needs to know. Radiographics. 2006; 26:23–39. PMID: 16418240.
Article15. Remy-Jardin M, Pistolesi M, Goodman LR, Gefter WB, Gottschalk A, Mayo JR, et al. Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology. 2007; 245:315–329. PMID: 17848685.
Article16. Ozsu S, Karaman K, Mentese A, Ozsu A, Karahan SC, Durmus I, et al. Combined risk stratification with computerized tomography/echocardiography and biomarkers in patients with normotensive pulmonary embolism. Thromb Res. 2010; 126:486–492. PMID: 20920821.17. Quiroz R, Kucher N, Schoepf UJ, Kipfmueller F, Solomon SD, Costello P, et al. Right ventricular enlargement on chest computed tomography: prognostic role in acute pulmonary embolism. Circulation. 2004; 109:2401–2404. PMID: 15148278.18. Kang DK, Thilo C, Schoepf UJ, Barraza JM Jr, Nance JW Jr, Bastarrika G, et al. CT signs of right ventricular dysfunction: prognostic role in acute pulmonary embolism. JACC Cardiovasc Imaging. 2011; 4:841–849. PMID: 21835376.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Compression of the Right Pulmonary Artery by a Massive Descending Aortic Aneurysm Causing Bilateral Perfusion Defects on Pulmonary Scintigraphy
- Clinical Outcome Related to Diagnosis of Saddle Pulmonary Embolism using Computed Tomographic Angiography in an Emergency Department
- Comparison of Contrast-enhanced Spiral CT Scan and Pulmonary Angiogra p hy in Diagnosing Pulmonary Embolism: An Experimental Study in Pig Models
- Measurements of thoracic aorta and pulmonary artery diameter by computed tomography in normal Korean adults
- Unilateral Absence of a Pulmonary Artery: Report of 3 cases
