A Case of Septic Pulmonary Embolism Associated with MRSA Infective Endocarditis
- Affiliations
-
- 1Department of Internal Medicine, DMC Bundang Jesaeng Hospital, Seongnam, Korea. jychin@dmc.or.kr
- 2Department of Chest Surgery, DMC Bundang Jesaeng Hospital, Seongnam, Korea.
- 3Department of Diagnostic Radiology, DMC Bundang Jesaeng Hospital, Seongnam, Korea.
- 4Department of Radiology, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea.
- 5Department of Anatomical Pathology, Hallym University College of Medicine, Seoul, Korea.
Abstract
- Septic pulmonary embolism is the process in which an infected thrombus becomes detached from its site of origin and lodges in a pulmonary artery, and is usually associated with infective endocarditis, especially right-sided, or infection-associated with indwelling catheters, peripheral septic thrombophlebitis, and periodontal diseases, etc. Here, we report a case of septic pulmonary embolism associated with tricuspid valve infective endocarditis. A 23-year-old female was admitted to our hospital, due to fever, sore throat, and myalgia. In her past medical history, she had undergone a surgical operation for closure of a ventricular septal defect, but was informed that the operation resulted in an incomplete closure. The initial chest radiograph demonstrated multiple rounded, parenchymal nodules in various sizes; several nodules had central lucency suggesting cavitations. Echocardiography demonstrated a large vegetation attached to the septal tricuspid valve leaflet, extending from right ventricular inflow tract to outflow tract. Computed tomography of thorax revealed bilateral peripheral nodules and wedge-shaped consolidation at various sizes, mostly accompanied by cavitations.
MeSH Terms
Figure
-

Figure 1 The chest radiograph shows multiple cavitary nodules (arrows) in both lungs. Also note parenchymal consolidation in right lower lung zone.
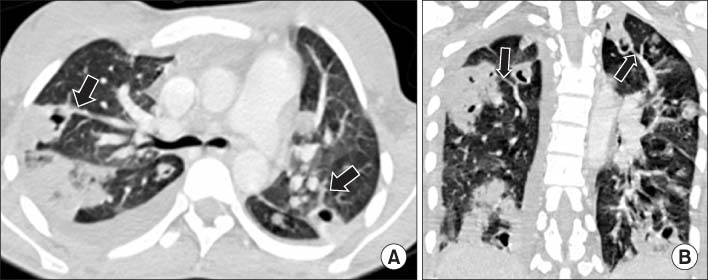
Figure 2 (A) The chest CT scan reveals bilateral peripheral nodules and wedge-shaped consolidation with various size. Some of the lesions show connection with pulmonary vessels (so-called feeding vessel sign, arrows), and this suggests septic emboli. Also note right pleural effusion. (B) The coronal reformatted CT image shows multiple nodules and areas of consolidation in almost all lobes. These parenchymal lesions are mainly located in peripheral lungs and connected with pulmonary vessels (arrows).

Figure 3 Transverse contrast-enhanced CT scan (mediastinal window setting) shows cardiomegaly and large filling defect in right ventricle (arrow), which is declared later as vegetation attached to septal tricuspid valve leaflet on echocardiographic examination.
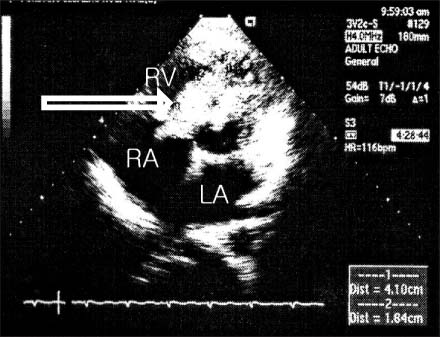
Figure 4 Echocardiogram shows a huge vegetation (41.0×18.4 mm) (arrow) attached to right ventricular side of septal tricuspid valve leaflet, extending from right ventricular inflow track to outflow tract (parasternal short axis view, arrow). LA: left atrium; RV: right ventricle; RA: right atrium.
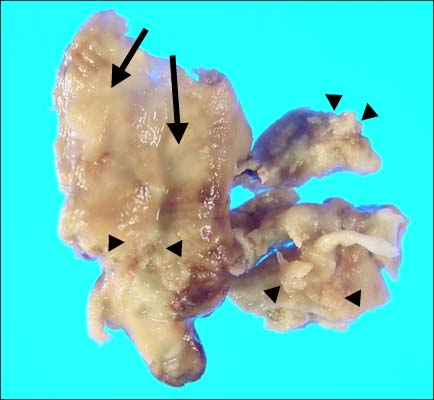
Figure 5 Gross findings of abnormal tissue resected by surgery (size 4×2.5×2 cm) showing irregularly shaped lesions (vegetation) (arrow head) attached to relatively smooth surfaced portion (diseased valve) (arrow).
Reference
-
1. Fred HL, Harle TS. Septic pulmonary embolism. Am Fam Physician GP. 1970. 1:81–87.2. Cook RJ, Ashiton RW, Aughenbaugh GL, Ryu JH. Septic pulmonary embolism: presenting features and clinical course of 14 patients. Chest. 2005. 128:162–166.3. Huang RM, Naidich DP, Lubat E, Schinella R, Garay SM, McCauley DI. Septic pulmonary emboli: CT-radiographic correlation. AJR Am J Roentgenol. 1989. 153:41–45.4. Rossi SE, Goodman PC, Franquet T. Nonthrombotic pulmonary emboli. AJR Am J Roentgenol. 2000. 174:1499–1508.5. Karchmer AW. Libby P, Bonow RO, Mann DL, Zipes DP, editors. Chapter 63. Infective endocarditis. Braunwald's heart disease: a textbook of cardiovascular medicine. 2007. 8th ed. Philadelphia: Saunders Elsevier;1713–1738.6. Webb DW, Thadepalli H. Hemoptysis in patients with septic pulmonary infarcts from tricuspid endocarditis. Chest. 1979. 76:99–100.7. Han D, Lee KS, Franquet T, Müller NL, Kim TS, Kim H, et al. Thrombotic and nonthrombotic pulmonary arterial embolism: spectrum of imanging findings. Radiographics. 2003. 23:1521–1539.8. Kuhlman JE, Fishman EK, Teigen C. Pulmonary septic emboli: diagnosis with CT. Radiology. 1990. 174:211–213.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mechanical Thrombectomy for Septic Embolism Secondary to Staphylococcus lugdunensis Bacteremia without Infective Endocarditis: A Case Report
- A Case of Hemophilus Paraphrophilus Endocarditis with Cerebral Embolism and Hemorrhage
- A Case of Tricuspid Valve Endocarditis with Pulmonary Embolism in a Drug Addict
- Acute Pulmonary Embolism Caused by Subacute Infective Endocarditis of the Tricuspid Valve
- A Case of Right Ventricular Infundibular and Pulmonic Valve Infective Endocarditis
