Malignant Mesothelioma Presenting as Large Neck Mass
- Affiliations
-
- 1Department of Radiology, The Catholic University of Korea College of Medicine, Seoul, Korea. hskimsph@catholic.ac.kr
- 2Department of Pulmonology, The Catholic University of Korea College of Medicine, Seoul, Korea.
- 3Department of Pathology, The Catholic University of Korea College of Medicine, Seoul, Korea.
Abstract
- Malignant mesothelioma is the most common primary malignant tumor involving pleura, but its diagnosis is difficult to determine by pathology in addition to the fact that it is rare. We present an unusual case of malignant mesothelioma, which initially presented as large neck mass contrary to the more common presentation of a rind like growth along the pleura demonstrated on imaging and by pathologic findings.
Keyword
MeSH Terms
Figure
-
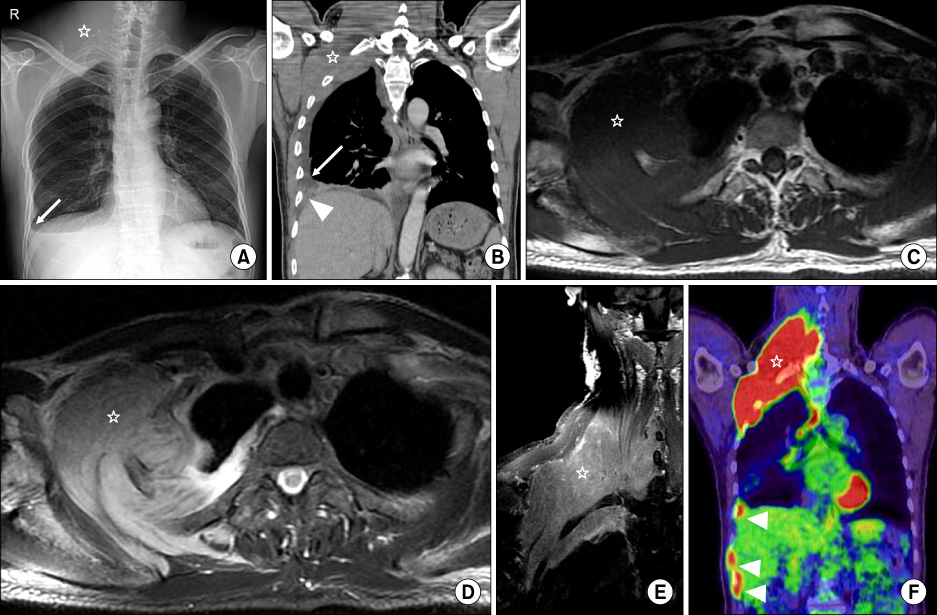
Figure 1 Images of malignant mesothelioma. Chest radiography (A) shows large soft tissue mass (☆) in right lower neck and right apex and small pleural effusion (arrow) in right costophrenic sulcus. There is no definite displacement or destruction of rib and contracture of right hemithorax. Contrast enhanced coronal CT image (B) reveals large muscle density malignant mesothelioma (☆) in right lower neck and right apex through rib cages. Mild pleural thickening (arrow head) and small pleural effusion (arrow) are also seen. The mass (☆) shows iso-signal intensity on T1 weighted axial MR image (C) and high signal intensity on T2 weighted image (D) with good contrast enhancement on coronal T1 weighted image (E). Soft tissue contrast between tumor and adjacent soft tissue is superior in MR than CT. Coronal PET image (F) reveals the intense uptake (SUV=9.6) of large malignant mass (☆) and small pleural nodules (arrow heads). SUV: standardized uptake valve.
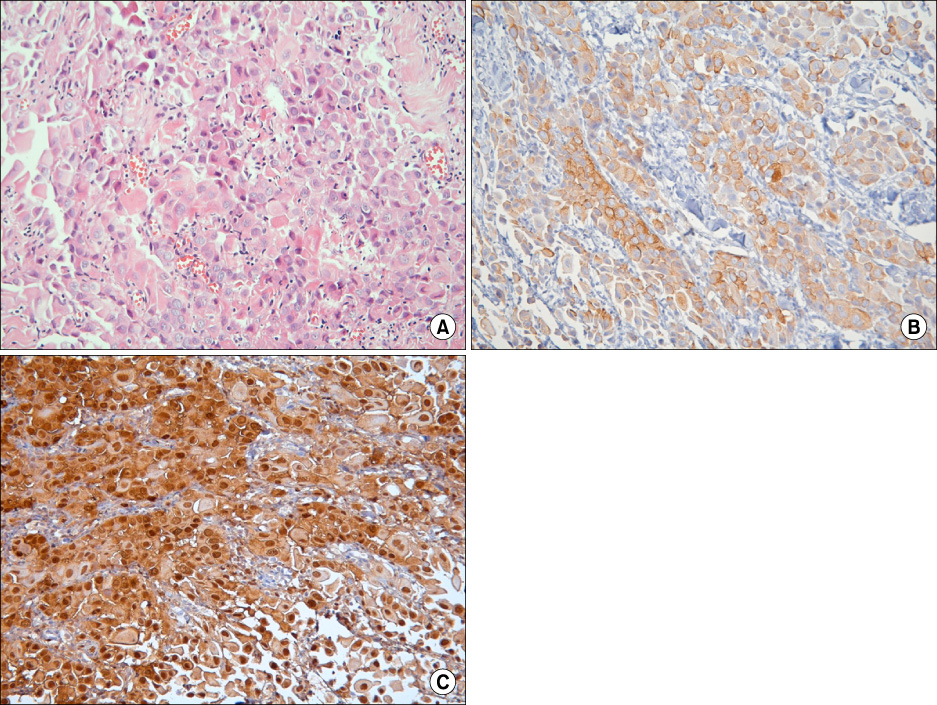
Figure 2 Histology of malignant mesothelioma. The tumor is composed of diffuse asheets of round to polygonal cells (H&E stain, ×200) (A). Immunohistochemical stains by CK 5/6 (B) and calretinin (C) show strong and diffuse cytoplasmic immunoreactivity in the tumor cells.

Figure 3 Follow up chest radiograph after 19 months shows regression of large neck mass and bilateral pleural effusions (arrows).
Reference
-
1. Attanoos RL, Gibbs AR. Pathology of malignant mesothelioma. Histopathology. 1997. 30:403–418.2. Gill RR, Gerbaudo VH, Jacobson FL, Trotman-Dickenson B, Matsuoka S, Hunsaker A, et al. MR imaging of benign and malignant pleural disease. Magn Reson Imaging Clin N Am. 2008. 16:319–339.3. Barreiro TJ, Katzman PJ. Malignant mesothelioma: a case presentation and review. J Am Osteopath Assoc. 2006. 106:699–704.4. Price B. Analysis of current trends in United States mesothelioma incidence. Am J Epidemiol. 1997. 145:211–218.5. Wang ZJ, Reddy GP, Gotway MB, Higgins CB, Jablons DM, Ramaswamy M, et al. Malignant pleural mesothelioma: evaluation with CT, MR imaging, and PET. Radiographics. 2004. 24:105–119.6. Kawashima A, Libshitz HI. Malignant pleural mesothelioma: CT manifestations in 50 cases. AJR Am J Roentgenol. 1990. 155:965–969.7. Truong MT, Marom EM, Erasmus JJ. Preoperative evaluation of patients with malignant pleural mesothelioma: role of integrated CT-PET imaging. J Thorac Imaging. 2006. 21:146–153.8. Beer TW, Buchanan R, Matthews AW, Stradling R, Pullinger N, Pethybridge RJ. Prognosis in malignant mesothelioma related to MIB 1 proliferation index and histological subtype. Hum Pathol. 1998. 29:246–251.9. Pistolesi M, Rusthoven J. Malignant pleural mesothelioma: update, current management, and newer therapeutic strategies. Chest. 2004. 126:1318–1329.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of primary malignant mesothelioma of tunica vaginalis testis
- Two cases of malignant mesothelioma of the peritoneum and pericardium
- Fine needle aspiration cytology of malignant epithelial mesothelioma of the peritoneum
- Malignant Mesothelioma Causing Bloody Pleural Effusion
- Malignant Mesothelioma Presenting as a Giant Chest, Abdominal and Pelvic Wall Mass
