A Case of Mediastinal Teratoma Associated with Elevated Tumor Marker in Chronic Empyema
- Affiliations
-
- 1Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea. son30243@hanmail.net
- 2Department of Pathology, Dong-A University College of Medicine, Busan, Korea.
- 3Department of Radiology, Dong-A University College of Medicine, Busan, Korea.
- 4Department of Thoracic and Cardiovascular Surgery, Dong-A University College of Medicine, Busan, Korea.
Abstract
- Most mediastinal teratomas are histologically well-differentiated tumors and benign. The majority of patients with a mediastinal teratoma are asymptomatic and their tumors are usually discovered incidentally on chest radiography. On rare occasions this tumor will rupture spontaneously into the adjacent organs. A 72-year-old female patient was admitted for dyspnea and she had a multiloculated pleural effusion in the left lung field. Although repeated pleural biopsy and pleural fluid cytology did not prove the presence of malignancy, we assumed that this was a malignant effusion because it revealed consistently high levels of carcinoembryonic antigen and carbohydrate antigen 19-9, and the chest CT scan did not show typical fat or bone density in the mass. Secondary infection and an uncontrolled septic condition due to pleural empyema finally compelled the patient to undergo a surgical operation. Mature teratoma was the final diagnosis and she has done well without recurrence for 2 months.
Keyword
MeSH Terms
Figure
-
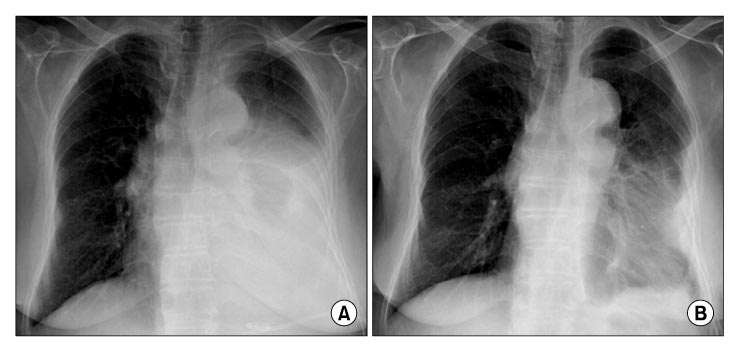
Figure 1 Chest radiograph on admission (A) shows large amount of left pleural effusion, and improved finding 20 days after removal of mediastinal teratoma and effusion (B).

Figure 2 Chest computed tomography (CT) on admission (A) shows large amount of multiloculated left pleural effusion with atelectatic change of left lung. A lobulated soft tissue density lesion within mediastinal pleural effusion and diffuse pleural thickening are seen. Chest CT after 6 months (B) shows no interval change of multiloculated left pleural effusion with internal soft tissue density lesion, and pleural thickening. Note newly developed pericardial and right pleural effusion.

Figure 3 The histologic findings of specimens are consistent with teratoma. The cystic area (A) is lined by keratinized stratified squamous epithelium (H&E stain, ×20). The solid area (B) is composed of heterogeneous mature tissues and organized structures, including pancreas tissue, muscle, cartilage and dilated glandular structures (H&E stain, ×100). Immunohistochemical stains of solid area (C) demonstrate positive staining for carcinoembryonic antigen (CEA).
Reference
-
1. Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest. 2005. 128:2893–2909.2. Kimura C, Kamiyoshihara M, Sakata K, Itoh H, Morishita Y. Mediastinal mature teratoma perforating into the lung with elevated serum carbohydrate antigen 19-9 (CA19-9) levels: report of a case. Kyobu Geka. 2003. 56:247–250.3. Ha ES, Hur GY, Jung KH, Lee SY, Jo WM, Lee SY, et al. Teratoma presenting as an unilateral mediastinal ma ss with contralateral pleural effusion. Tuberc Respir Dis. 2006. 60:347–352.4. Jeon JB, Hwan CC, Moon TH, Cho JW, Ryu JS, Kwak SM, et al. Spontaneuos rupture of mediastinal teratoma into adjacent tissue. Tuberc Respir Dis. 1999. 47:400–405.5. Lee TH, Lee SE, Baik JJ, Chung Y. A case of mediastinal teratoma complicated by spontaneous ruptured into pleural cavity. Tuberc Respir Dis. 1999. 47:265–271.6. Oomman A, Santhosham R, Vijayakumar C, Jayaraman S, Ramachandran P, Kumar S. Anterior mediastinal teratoma presenting as cardiac tamponade. Indian Heart J. 2004. 56:64–66.7. Pack HM, Kim ES, Kang JH, Jee HO. Anterior mediastinal teratoma which complicated empyema. Korean J Thorac Cardiovasc Surg. 1988. 21:535–540.8. Light RW. Clinical practice: pleural effusion. N Engl J Med. 2002. 346:1971–1977.9. Poe RH, Israel RH, Utell MJ, Hall WJ, Greenblatt DW, Kallay MC. Sensitivity, specificity, and predictive values of closed pleural biopsy. Arch Intern Med. 1984. 144:325–328.10. Gu P, Huang G, Chen Y, Zhu C, Yuan J, Sheng S. Diagnostic utility of pleural fluid carcinoembryonic antigen and CYFRA 21-1 in patients with pleural effusion: a systematic review and meta-analysis. J Clin Lab Anal. 2007. 21:398–405.11. Nagata K, Iwasaki Y, Nakanishi M, Natsuhara A, Harada H, Yokomura I, et al. A case of mediastinal teratoma with elevated serum tumor marker levels. Nihon Kokyuki Gakkai Zasshi. 2002. 40:50–54.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Medistinal Teratoma with Pleural and Pericardial Effusion Teratoma with Pleural and Pericardial Effusion
- Rapidly Grown Huge Mediastinal Benign Teratoma: one case report
- Treatment of Huge Chronic Tuberculous Empyema with Cardiopulmonary Dysfunction: 1 case report
- Treatment of Mediastinal Growing Teratoma Syndrome: A case report
- Ruptured Mediastinal Benign Teratoma with Focal Emphysema: A Case Report
