Utility of B-type Natriuretic Peptide in Patients with Acute Respiratory Distress Syndrome
- Affiliations
-
- 1Divison of Respiratory & Critical Care Medicine, Department of Internal Medicine, Kangnam St. Mary's Hospital, The Catholic University of Korea, Korea. youngkim@catholic.ac.kr
- 2Divison of Cardiology Medicine, Department of Internal Medicine, Kangnam St. Mary's Hospital, Seoul, Korea.
Abstract
-
BACKGROUND: B-type natriuretic peptide (BNP) has been shown to be strong mortality predictors in a wide variety of cardiovascular syndromes. Little is known about BNP in patients with acute respiratory distress syndrome (ARDS). We studied whether BNP can predict mortality in patients with ARDS.
METHOD: Echocardiographic study was done to all patients with ARDS, and we excluded patient with low ejection fraction (less than 50%) or showing any features of diastolic dysfunction. 47 patients were enrolled between December, 2003 and February, 2006. Parameters including BNP were obtained within 24h hours at the time of enrollment.
RESULT: Mean BNP concentrations and APACHE II scores differed between the survivors and nonsurvivors (BNP, 219.5 +/- 57.7 pg/mL vs 492.3 +/- 88.8 pg/mL; p=0.013, APACHE II score, 17.4 +/- 1.6 vs 23.1 +/- 1.3, p=0.009, respectively). With the use of the threshold value for BNP of 585 pg/mL, the specificity for the prediction of mortality was 94%. The threshold value for APACHE II of 15.5 showed sensitivity of 87%. 'APACHE II + 11xlogBNP' showed sensitivity 63%, and specificity 82%, using threshold value for 46.14.
CONCLUSION
BNP concentrations and APCHE II scores were more elevated in nonsurvivors than survivors in patients with ARDS who have normal ejection fraction. BNP can predict mortality. Further study should be done.
Keyword
MeSH Terms
Figure
-
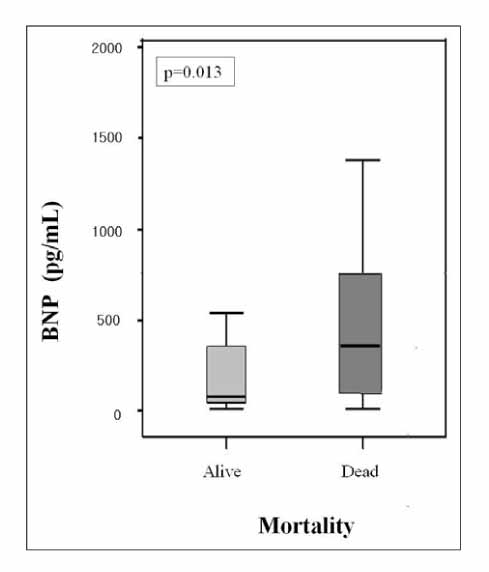
Figure 1 Box and whiskers plots of median B-type natriuretic peptide (BNP) concentrations among surviving patients vs. those dying during the study. The median BNP concentrations among those dying were significantly higher than those surviving (p = 0.013).

Figure 2 Box and whiskers plots of median acute physiology and chronic health evaluation (APACHE) II scores among surviving patients vs. those dying during the study. The median APACHE II scores among those dying were significantly higher than those surviving (p = 0.009).
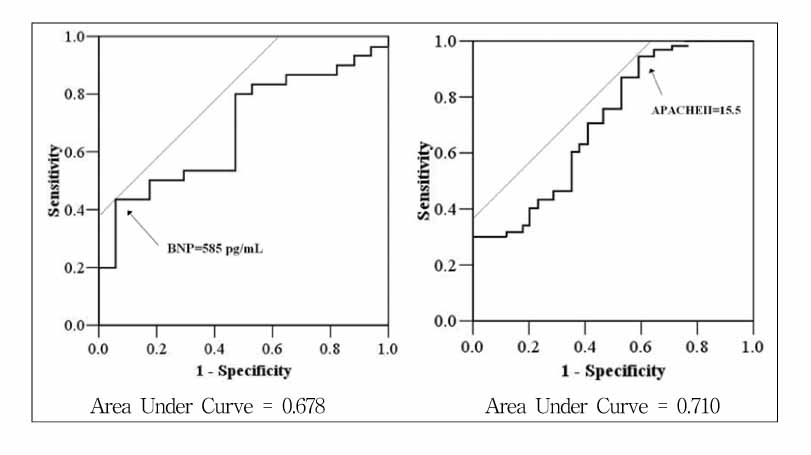
Figure 3 Receiver operating characteristic curve for BNP (left) APACHE II score (right) for the prediction of mortality. BNP: B-type natriuretic peptide; APACHE: Acute Physiology and Chronic Health Evaluation
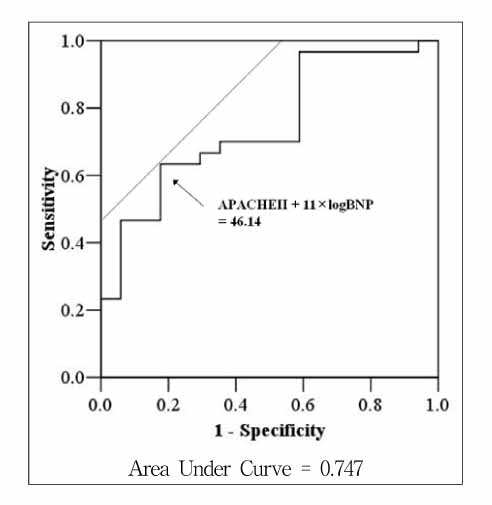
Figure 4 Receiver operating characteristic curve for 'APACHE II score + 11×log BNP' for the prediction of mortality. BNP: B-type natriuretic peptide; APACHE: Acute Physiology and Chronic Health Evaluation
Reference
-
1. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002. 347:161–167.2. Vasan RS, Benjamin EJ, Larson MG, Leip EP, Wang TJ, Wilson PW, et al. Plasma natriuretic peptides for community screening for left ventricular hypertrophy and systolic dysfunction: the Framingham heart study. JAMA. 2002. 288:1252–1259.3. Maisel AS, Koon J, Krishnaswamy P, Kazenegra R, Clopton P, Gardetto N, et al. Utility of B-natriuretic peptide as a rapid, point-of-care test for screening patients undergoing echocardiography to determine left ventricular dysfunction. Am Heart J. 2001. 141:367–374.4. Omland T, Aakvaag A, Bonarjee VV, Caidahl K, Lie RT, Nilsen DW, et al. Plasma brain natriuretic peptide as an indicator of left ventricular systolic function and long-term survival after acute myocardial infarction. Comparison with plasma atrial natriuretic peptide and N-terminal proatrial natriuretic peptide. Circulation. 1996. 93:1963–1969.5. Krishnaswamy P, Lubien E, Clopton P, Koon J, Kazanegra R, Wanner E, et al. Utility of B-natriuretic peptide levels in identifying patients with left ventricular systolic or diastolic dysfunction. Am J Med. 2001. 111:274–279.6. Hammerer-Lercher A, Neubauer E, Muller S, Pachinger O, Puschendorf B, Mair J. Head-to-head comparison of N-terminal pro-brain natriuretic peptide, brain natriuretic peptide and N-terminal pro-atrial natriuretic peptide in diagnosing left ventricular dysfunction. Clin Chim Acta. 2001. 310:193–197.7. Mair J, Hammerer-Lercher A, Puschendorf B. The impact of cardiac natriuretic peptide determination on the diagnosis and management of heart failure. Clin Chem Lab Med. 2001. 39:571–588.8. Bettencourt P. NT-proBNP and BNP: biomarkers for heart failure management. Eur J Heart Fail. 2004. 6:359–363.9. Yeo KT, Wu AH, Apple FS, Kroll MH, Christenson RH, Lewandrowski KB, et al. Multicenter evaluation of the Roche NT-proBNP assay and comparison to the Biosite Triage BNP assay. Clin Chim Acta. 2003. 338:107–115.10. Maeder M, Ammann P, Rickli H, Diethelm M. Elevation of B-type natriuretic peptide levels in acute respiratory distress syndrome. Swiss Med Wkly. 2003. 133:515–518.11. Mitaka C, Hirata Y, Nagura T, Tsunoda Y, Itoh M, Amaha K. Increased plasma concentrations of brain natriuretic peptide in patients with acute lung injury. J Crit Care. 1997. 12:66–71.12. Tung RH, Garcia C, Morss AM, Pino RM, Fifer MA, Thompson BT, et al. Utility of B-type natriuretic peptide for the evaluation of intensive care unit shock. Crit Care Med. 2004. 32:1643–1647.13. Jefic D, Lee JW, Jefic D, Savoy-Moore RT, Rosman HS. Utility of B-type natriuretic peptide and N-terminal pro B-type natriuretic peptide in evaluation of respiratory failure in critically ill patients. Chest. 2005. 128:288–295.14. Bal L, Thierry S, Brocas E, Van de Louw A, Pottecher J, Hours S, et al. B-type natriuretic peptide (BNP) and N-terminal-proBNP for heart failure diagnosis in shock or acute respiratory distress. Acta Anaesthesiol Scand. 2006. 50:340–347.15. Garcia MJ, Thomas JD, Klein AL. New Doppler echocardiographic applications for the study of diastolic function. J Am Coll Cardiol. 1998. 32:865–875.16. Vieillard-Baron A, Prin S, Chergui K, Dubourg O, Jardin F. Echo-Doppler demonstration of acute cor pulmonale at the bedside in the medical intensive care unit. Am J Respir Crit Care Med. 2002. 166:1310–1319.17. Feigenbaum H, Armstrong WF, Ryan T. Feigenbaum's Echocardiography. 2005. 6th ed. Philadelphia: Lippincott Williams & Wilkins;209.18. Phua J, Lim TK, Lee KH. B-type natriuretic peptide: issues for the intensivist and pulmonologist. Crit Care Med. 2005. 33:2094–2013.19. Berendes E, Van Aken H, Raufhake C, Schmidt C, Assmann G, Walter M. Differential secretion of atrial and brain natriuretic peptide in critically ill patients. Anesth Analg. 2001. 93:676–682.20. Karmpaliotis D, Kirtane AJ, Ruisi CP, Polonsky T, Malhotra A, Talmor D, et al. Diagnostic and prognostic utility of brain natriuretic Peptide in subjects admitted to the ICU with hypoxic respiratory failure due to noncardiogenic and cardiogenic pulmonary edema. Chest. 2007. 131:964–971.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biomarkers in Heart Failure: Focus on B-type Natriuretic Peptide
- B-type natriuretic peptide may have a role in the management of patent ductus arteriosus
- B-type natriuretic peptide in anesthesia practice to predict adverse cardiovascular outcomes
- Clinical Implication of B-type Natriuretic Peptide in the Elderly
- Treatment of Acute Respiratory Distress Syndrome
