A Case of Multiple Endobronchial Metastases from Prostatic Carcinoma
- Affiliations
-
- 1Division of Pulmonology, Department of Internal Medicine, Chungnam National University Hospital & Cancer Research Institute, Daejeon, South Korea. jokim@cnu.ac.kr
- 2Department of Pathology, Chungnam National University Hospital & Cancer Research Institute, Daejeon, South Korea.
- 3Department of Urology, Chungnam National University Hospital & Cancer Research Institute, Daejeon, South Korea.
Abstract
- The lung is the most common site for the metastasis of extrapulmonary malignant tumors. However, endobronchial metastases (EBM) from extrapulmonary malignant tumors are rare. The most common extrathoracic malignancies associated with EBM are the breast, renal and colorectal carcinomas. Lung metastasis from prostate cancer is often encountered but EBM is rare. We report a 74-year old man with endobronchial metastases from prostatic carcinoma presented with cough. The diagnosis of prostatic cancer and the endobronchial metastasis were confirmed by immunohistological staining with the prostate specific antigen. Hormonal therapy (lutenizing hormone releasing hormone agonist) was applied to this patient.
MeSH Terms
Figure
-

Figure 1 Chest X-ray showed no definitive parenchymal lesions. Pleural effusion was located in right lung.
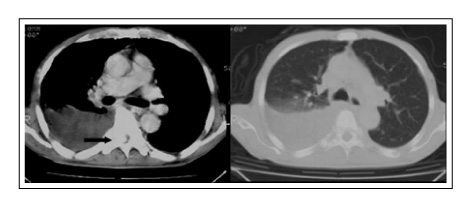
Figure 2 Chest CT scan revealed loculated pleural effusion on right side. There was no definitive parenchymal lesion and no enlarged lymph nodes. There was bony mentastasis in thoracic vertebrae producing cord compression. (arrow).
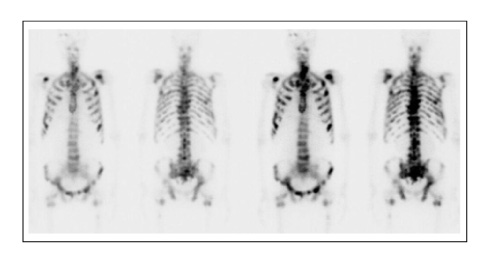
Figure 3 Whole body bone scan showed multiple bony metastases.

Figure 4 Pelvic CT showed normal prostate.
Figure 5 Bronchoscopic finding showed multiple nodular masses in trachea (A), right (B) and left main bronchus (C), and single polypoid mass in right middle lobe brochus (right lower panel).
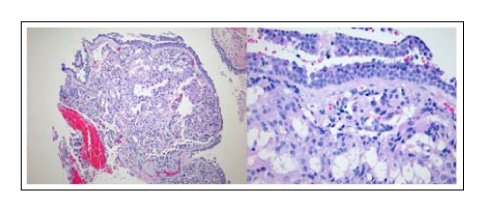
Figure 6 Representative hematoxylin/eosin-stained sections of the endobronchial mucosal lesion showed diffuse infiltration of well differentiated adenocarcinoma cells. (Left panel ×40, Right panel ×200).

Figure 7 Representative hematoxylin/eosin-stained sections of the prostate tissue showed neoplastic proliferation of glandular epithelial cells (×100).
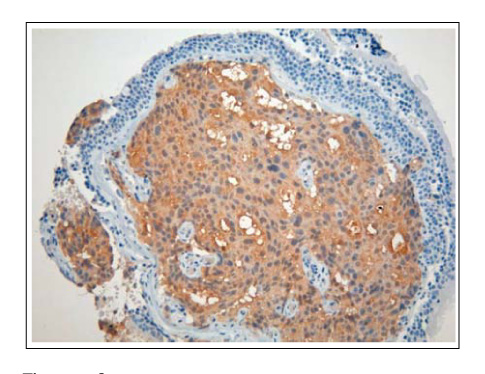
Figure 8 Representative light microscopy of PSA-positive cells in the bronchial tissue. The brown color indicates PSA-positive cells (×200).
Reference
-
1. Braman SS, Witcomb ME. Endobronchial metastases. Arch Intern Med. 1975. 135:543–547.2. Baumgartner WA, Mark JB. Metastatic malignancies from distant sites to the tracheobronchial tree. J Thorac Cardiovasc Surg. 1980. 79:499–503.3. Pass HI, Donigtom JS. DeVita VT, Hellman S, Rosenberg SA, editors. Metastatic cancer to the lung. Cancer: principles and practice of oncology. 1997. Philadelphia: Lippincot-Rowen Publishers;2536–2550.4. Scoggins WG, Witten JA Jr, Texter JH Jr, Hazra TA. Endobronchial metastasis from prostatic cancer in patients with renal cell carcinoma. Urology. 1978. 12:207–209.5. Stranzl H, Gabor S, Mayer R, Prettenhofer U, Wurzinger G, Hackl A. Fractionated intraluminal HDR 192Ir brachytherapy as palliative treatment in patients with endobronchial metastases from nonbronchogenic primaries. Strahlenther Onkol. 2002. 178:442–445.6. Lee DW, Ro JY, Sahin AA, Lee JS, Ayala AG. Mucinous-adenocarcinoma of the prostate with endobronchial metastasis. Am J Clin Pathol. 1990. 94:641–645.7. Quantrill SJ, Burt PA, Barber PV, Stout R. Treatment of endobronchial metastases with intraluminal radiotherapy. Respir Med. 2000. 94:369–372.8. Heitmiller RF, Marasco WJ, Hruban RH, Marsh BR. Endobronchial metastasis. J Thorac Cardiovasc Surg. 1993. 106:537–542.9. Katsimbri PP, Bamias AT, Froudarakis ME, Peponis IA, Constantopoulos SH, Pavlidis NA. Endobronchial metastases secondary to solid tumors: report of eight cases and review of the literature. Lung Cancer. 2000. 28:163–170.10. Salud A, Porcel JM, Rovirosa A, Bellmunt J. Endobronchial metastatic disease: analysis of 32 cases. J Surg Oncol. 1996. 62:249–252.11. Poe RH, Israel RH, Qazi R, Ortiz C, Marin MG, Dale RC, et al. Sensitivity, specificity, and predictive values of bronchoscopy in neoplasm metastatic to the lung. Chest. 1985. 88:84–88.12. Diaz G, Jimenez D, Dominguez-Reboiras S, Carrillo F, Perez-Rodriguez-E . Yield of bronchoscopy in the diagnosis of neoplasm metastatic to lung. Respir Med. 2003. 97:27–29.13. Nagji M, Tabei SZ, Castro A, Chu TM, Murphy GP, Wang MC, et al. Prostatic specific antigen: an immunohistochemical marker for prostatic neoplasm. Cancer. 1981. 48:1229–1232.14. Lalli C, Gogia H, Raju L. Multiple endobronchial metastases from carcinoma of prostate. Urology. 1983. 21:164–165.15. Carlin BW, Harrel JH, Olson LK, Moser KM. Endobronchial metastases due to colorectal carcinoma. Chest. 1989. 96:1110–1114.
