A Case of Delayed Response of Tumorous type of Endobronchial Tuberculosis to Antituberculosis Treatment
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. shimts@amc.seoul.kr
Abstract
- Pulmonary tuberculomas show variable responses to treatment, with some even increasing in size after treatment. To date, however, no data have been reported on the response of tumorous type of endobronchial tuberculosis (EBTB-T) to treatment observed both bronchoscopically and histologically. We report a case of bacteriologically- and biopsy-proven EBTB-T that showed delayed response to anti-tuberculosis treatment. Even after EBTB-T was treated with antituberculosis drugs for 15 months, the bronchoscopic findings and the histologic findings of chronic granulomatous inflammation with caseation necrosis still remained. However, in fourteen months after the completion of treatment, the lesioneventually disappeared without further treatment.
MeSH Terms
Figure
-
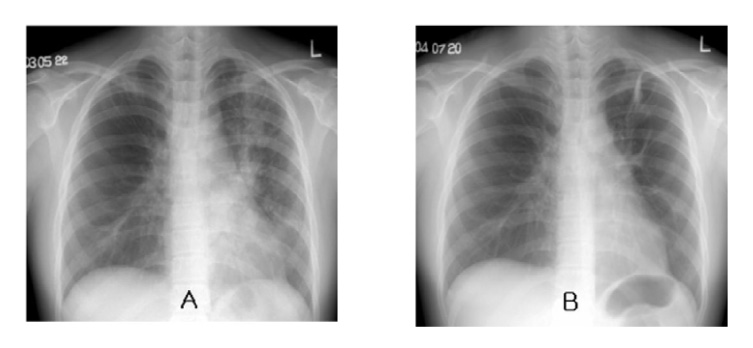
Figure 1 Chest radiographic findings A. Baseline chest radiography before treatment shows multifocal patchy air-space consolidation and multiple small nodular densities along bronchovascular bundle with subsegmental atelectasis in the left upper lobe. B. Chest radiography at treatment completion shows decreased extent of ill-defined nodular opacity and persistent fibrotic change with subsegmental atelectasis in the left upper lobe.
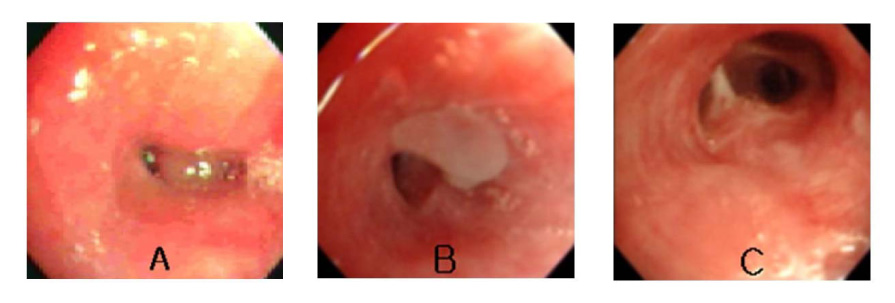
Figure 2 Bronchoscopic findings A. Baseline. A smooth-surfaced endobronchial mass obstructing anterior segmental bronchus of upper division of left upper lobe was seen. B. At treatment completion. A flesh-like soft tissue mass covered with whitish necrotic material was persistent at the same site with slightly decreased size. C. Fourteen months later after treatment completion. The mass disappeared and the anterior segmental bronchus of upper division of left upper lobe was patent with minimal fibrotic changes.
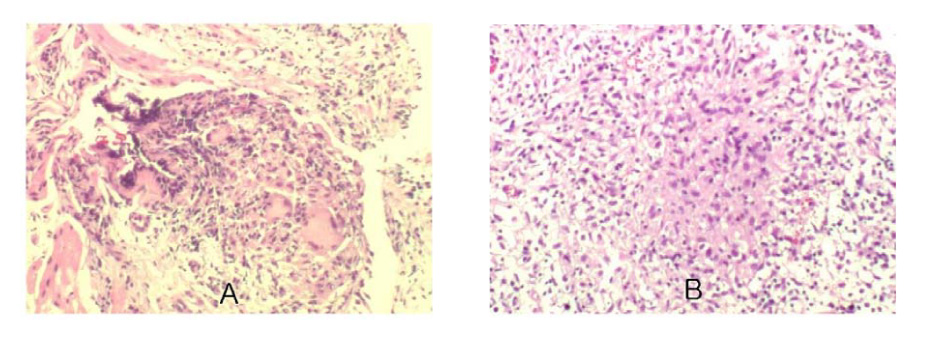
Figure 3 Microscopic findings (× 400) Baseline. Chronic granulomatous inflammation (TB PCR - positive) B. At treatment completion. Chronic granulomatous inflammation with caseating necrosis ( AFB - positive ).
Reference
-
1. Chung HS, Lee JH, Han SK, Shim YS, Kim KY, Han YC, et al. Classification of endobronchial tuberculois by the bronchoscopic feature. Tuberc Respir Dis. 1991. 38:108–115.2. Grenville-Mathers R. The natural history of so-called tuberculomas. J Thorac Surg. 1952. 23:251–252.3. Lee HS, Oh JY, Lee JH, Yoo CG, Lee CT, Kim YW, et al. Response of pulmonaray tuberculomas to anti-tuberculous treatment. Eur Respir J. 2004. 23:452–455.4. Shim YS. Endobronchial tuberculosis. Respirology. 1996. 1:95–106.5. Chung HS, Lee HH. Changes in bronchoscopic findings during treatment-course in active endobronchial tuberculosis. Tuberc Respir Dis. 1995. 42:25–34.6. Chung HS, Hyun IG, Han SK. Bronchoscopic electrocautery for airway obstruction in the tumorous type of endobronchial tuberculosis. Tuberc Respir Dis. 1991. 38:347–356.7. Song JH, Han SK, Heo IM. Clinical study on endobronchial tuberculosis. Tuberc Respir Dis. 1985. 32:276–282.8. Judd A. Tuberculous tracheobronchitis. J Thorac Surg. 1947. 16:512–519.9. Wishnitzer R, Eliraz A, Sternfeld M, Suher A, Knobler H. Endobronchial tuberculosis. Harefuah. 1989. 116:356–358.10. Smith LS, Schillaci RF, Sarlin RF. Endobronchial tuberculosis: serial fiberoptic bronchoscopy and natural history. Chest. 1987. 91:644–647.11. Han SK. Pulmonary tuberculosis. 1990. Seoul: Iljogak.12. Auerbach O. Pathology of tuberculosis as affected by antibiotics. Am J Surg. 1955. 89:627–636.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of tumorous type of endobronchial tuberculosis simulating bronchial adenoma
- A Case of Endobronchial Tuberculosis with Repeated Expectoration of Nodular Tissues
- Changes in Bronchoscopic Findings during Treatment-Course in Active Endobronchial Tuberculosis
- The Effect of Corticosteroid on the Treatment of Endobronchial Tuberculosis
- Bronchoscopic electrocautery for airway obstruction in the tumorous type of endobronchial tuberculosis
