J Korean Ophthalmol Soc.
2016 Jul;57(7):1126-1133. 10.3341/jkos.2016.57.7.1126.
Clinical Outcomes of Early Phacoemulsification after Laser Iridotomy in Acute Angle-closure Glaucoma
- Affiliations
-
- 1Department of Ophthalmology, Armed Forces DaeGu Hospital, Gyeongsan, Korea.
- 2Department of Ophthalmology, Hallym University College of Medicine, Chuncheon, Korea. kyungwlee@hanmail.net
- KMID: 2317574
- DOI: http://doi.org/10.3341/jkos.2016.57.7.1126
Abstract
- PURPOSE
To evaluate long-term change in intraocular pressure (IOP) in eyes undergoing laser iridotomy (LI) and early phacoemulsification after LI in patients with acute angle-closure glaucoma (AACG).
METHODS
The retrospective, comparative chart review included patients with AACG, Group A who underwent only LI and Group B who underwent early phacoemulsification within 1 month after LI. Patients were followed up on day 1; week 1; and months 1, 3, 6, and 12 after LI. IOP changes were studied.
RESULTS
This study included a total 99 eyes from 99 patients, 37 in group A and 62 in group B. The mean IOP were not significantly different between the two groups at the initial visit or 1 month later. However, group B showed a consistently lower mean IOP that that of group A at 3, 6, and 12 months (p= 0.003, <0.001, <0.001, respectively). The prevalence of IOP increase to greater than 21 mmHg was 3 (8.11%), 5 (13.51%), and 5 patients (13.51%) in group A and 0, 2 (5.41%), and 1 patients (1.61%) in group B at 3, 6, and 12 months, respectively. Group B showed a significantly lower prevalence of IOP increase (p = 0.050, 0.038, 0.026).
CONCLUSIONS
We found that patients treated with early phacoemulsification after LI had better outcomes of well-maintained IOP compared to those undergoing LI alone. For AACG patients with coexisting cataract, early phacoemulsification after LI can be considered as a reasonable treatment to maintain IOP.
MeSH Terms
Figure
-
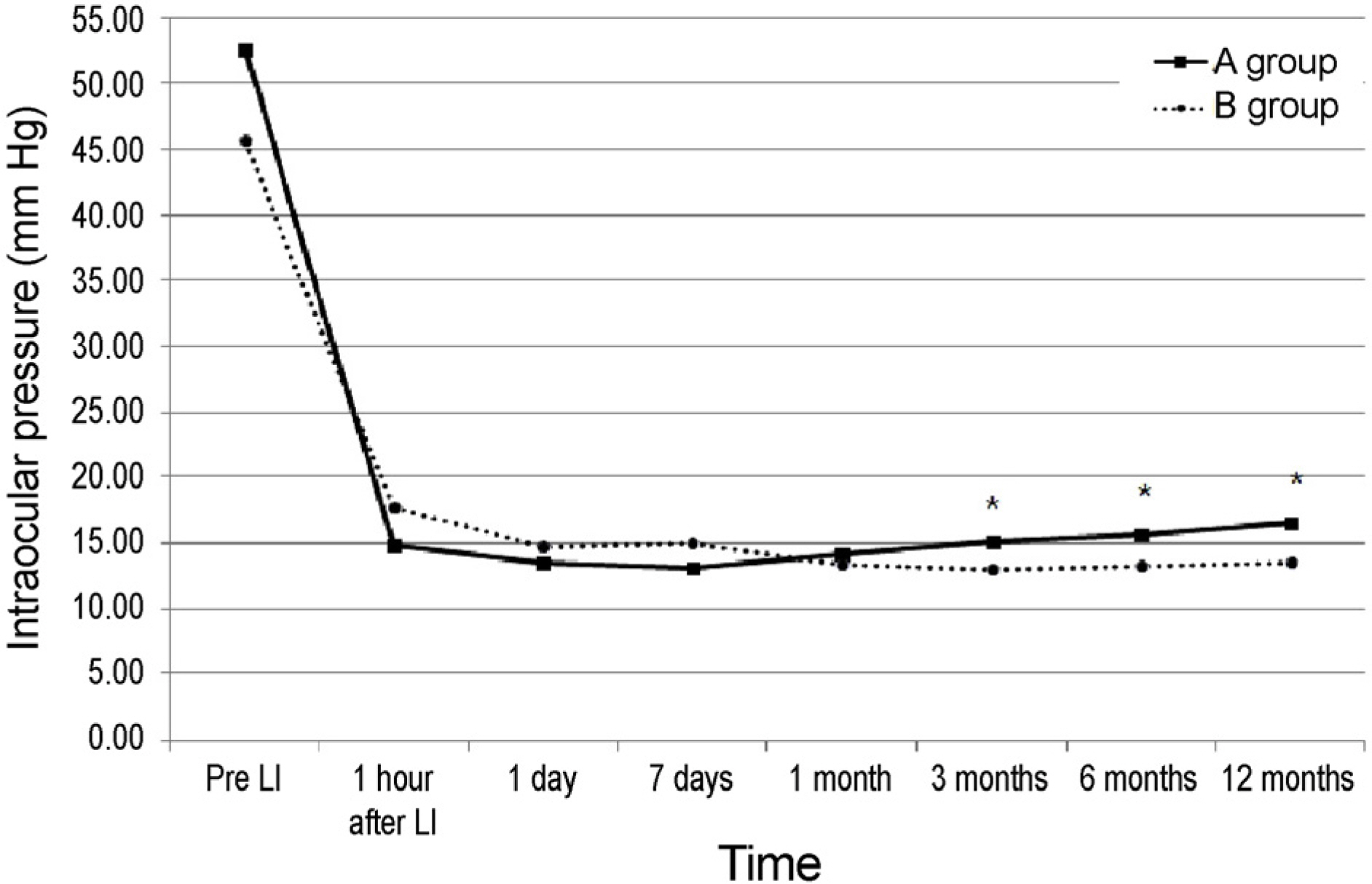
Figure 1. Change of mean intraocular pressure for the Group A and B. Group A was 37 patients who underwent only laser iridotomy (LI) and Group B was 62 patients who underwent early phacoemulsification after LI within 1 month. The mean intraocular pressure (IOP) between two groups were not significantly different at initial visit and 1 month. But group B showed consistently lower mean IOP that that of group A for the follow-up at 3, 6, 12 months (p = 0.003, <0.001, <0.001). * p < 0.05 by independent samples t-test.
Reference
-
References
1. Kim YY, Lee JH, Ahn MD, et al. Angle closure in the Namil study in central South Korea. Arch Ophthalmol. 2012; 130:1177–83.
Article2. Kim CS, Seong GJ, Lee NH, et al. Prevalence of primary open-abdominal glaucoma in central South Korea the Namil study. Ophthalmology. 2011; 118:1024–30.3. Quigley HA. Number of people with glaucoma worldwide. Br J Ophthalmol. 1996; 80:389–93.
Article4. Robin AL, Pollack IP. Argon laser peripheral iridotomies in the treatment of primary angleclosure glaucoma. abdominal follow-up. Arch Ophthalmol. 1982; 100:919–23.5. Salmon JF. abdominal intraocular pressure control after Nd-YAG laser iridotomy in chronic abdominal glaucoma. J Glaucoma. 1993; 2:291–6.6. Lam DS, Lai JS, Tham CC, et al. Argon laser peripheral iridoplasty versus conventional systemic medical therapy in treatment of acute primary abdominal glaucoma: a prospective, randomized, abdominalled trial. Ophthalmology. 2002; 109:1591–6.7. Aung T, Ang LP, Chan SP, Chew PT. Acute primary abdominal: long-term intraocular pressure outcome in Asian eyes. Am J Ophthalmol. 2001; 131:7–12.8. Ming Zhi Z, Lim AS, Yin Wong T. A pilot study of lens extraction in the management of acute primary abdominal glaucoma. Am J Ophthalmol. 2003; 135:534–6.9. Tarongoy P, Ho CL, Walton DS. Angle-closure glaucoma: the role of the lens in the pathogenesis, prevention, and treatment. Surv Ophthalmol. 2009; 54:211–25.
Article10. Hayashi K, Hayashi H, Nakao F, Hayashi F. Effect of cataract abdominal on intraocular pressure control in glaucoma patients. J Cataract Refract Surg. 2001; 27:1779–86.11. Jacobi PC, Dietlein TS, Lüke C, et al. Primary phacoemulsification and intraocular lens implantation for acute abdominal glaucoma. Ophthalmology. 2002; 109:1597–603.12. Pereira FA, Cronemberger S. Ultrasound biomicroscopic study of anterior segment changes after phacoemulsification and foldable intraocular lens implantation. Ophthalmology. 2003; 110:1799–806.
Article13. Chen YY, Chen YY, Sheu SJ, Chou P. The biometric study in abdominal stages of primary abdominal glaucoma. Eye (Lond). 2013; 27:1070–6.14. Shams PN, Foster PJ. Clinical outcomes after lens extraction for visually significant cataract in eyes with primary angle closure. J Glaucoma. 2012; 21:545–50.
Article15. Musch DC, Gillespie BW, Niziol LM, et al. Cataract extraction in the collaborative initial glaucoma treatment study: incidence, risk factors, and the effect of cataract progression and extraction on clinical and quality-of-life outcomes. Arch Ophthalmol. 2006; 124:1694–700.16. Lowe RF. Aetiology of the anatomical basis for primary abdominal glaucoma. Biometrical comparisons between normal eyes and eyes with primary abdominal glaucoma. Br J Ophthalmol. 1970; 54:161–9.17. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002; 86:238–42.
Article18. Chen Y, Bao YZ, Pei XT. Morphologic changes in the anterior chamber in patients with cortical or nuclear age-related cataract. J Cataract Refract Surg. 2011; 37:77–82.
Article19. Erie JG, Hodge DO, Gray DT. The incidence of primary abdominal glaucoma in Olmsted County, Minnesota. Arch Ophthalmol. 1997; 115:177–81.20. Ritch R, Lowe RF. Angle-closure glaucoma: therapeutic overview. Ritch R, Shields MB, Krupin T, editors. The Glaucomas: Glaucoma Therapy. 2nd ed.St Louis: Mosby;1996. p. 1521–31.21. Strorey JK, Phillips CL. Ocular dimensions in angle closure glaucoma. Br J Physiol Optics. 1971; 26:228–42.22. Nonaka A, Kondo T, Kikuchi M, et al. Cataract surgery for residual angle closure after peripheral laser iridotomy. Ophthalmology. 2005; 112:974–9.
Article23. Nonaka A, Kondo T, Kikuchi M, et al. Angle widening and abdominal of ciliary process configuration after cataract surgery for abdominal angle closure. Ophthalmology. 2006; 113:437–41.24. Lam DS, Leung DY, Tham CC, et al. Randomized trial of early phacoemulsification versus peripheral iridotomy to prevent abdominal pressure rise after acute primary angle closure. Ophthalmology. 2008; 115:1134–40.25. Dada T, Rathi A, Angmo D, et al. Clinical outcomes of clear lens extraction in eyes with primary angle closure. J Cataract Refract Surg. 2015; 41:1470–7.
Article26. Trikha S, Perera SA, Husain R, Aung T. The role of lens extraction in the current management of primary abdominal glaucoma. Curr Opin Ophthalmol. 2015; 26:128–34.27. Azuara-Blanco A, Burr JM, Cochran C, et al. The effectiveness of early lens extraction with intraocular lens implantation for the treatment of primary abdominal glaucoma (EAGLE): study abdominal for a randomized controlled trial. Trials. 2011; 12:133.
Article28. Sihota R, Lakshmaiah NC, Walia KB, et al. The trabecular abdominal in acute and chronic angle closure glaucoma. Indian J Ophthalmol. 2001; 49:255–9.29. Lee KM, Lee SH, Kim MS. Clinical results of phacoemulsification in eyes with acute abdominal glaucoma in the aspect of complications. J Korean Ophthalmol Soc. 2009; 50:44–50.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Phacoemulsification versus Laser Peripheral Iridotomy in Early Treatment of Acute Primary Angle-Closure Glaucoma
- Long-Term Intraocular Pressure Outcome in Fellow Eyes with Angle-Closure Glaucoma after Laser Iridotomy and Phacoemulsification
- Argon Laser Iridotomy
- Clinical Results of the Q-Switched Nd-YAG Laser Iridotomy
- Effect of YAG Laser Iridotomy on IOP in Chronic Angle-closure Glaucoma
