Acute Ischemic Stroke Involving Both Anterior and Posterior Circulation Treated by Endovascular Revascularization for Acute Basilar Artery Occlusion via Persistent Primitive Trigeminal Artery
- Affiliations
-
- 1Department of Neurosurgery, Kobe University Graduate School of Medicine, Kobe, Japan. taichiro.imahori@gmail.com
- KMID: 2315977
- DOI: http://doi.org/10.3340/jkns.2016.59.4.400
Abstract
- We report a case of acute ischemic stroke involving both the anterior and posterior circulation associated with a persistent primitive trigeminal artery (PPTA), treated by endovascular revascularization for acute basilar artery (BA) occlusion via the PPTA. An otherwise healthy 67-year-old man experienced sudden loss of consciousness and quadriplegia. Magnetic resonance imaging showed an extensive acute infarction in the right cerebral hemisphere, and magnetic resonance angiography showed occlusion of the right middle cerebral artery (MCA) and BA. Because the volume of infarction in the territory of the right MCA was extensive, we judged the use of intravenous tissue plasminogen activator to be contraindicated. Cerebral angiography revealed hypoplasia of both vertebral arteries and the presence of a PPTA from the right internal carotid artery. A microcatheter was introduced into the BA via the PPTA and revascularization was successfully performed using a Merci Retriever with adjuvant low-dose intraarterial urokinase. After treatment, his consciousness level and right motor weakness improved. Although persistent carotid-vertebrobasilar anastomoses such as a PPTA are relatively rare vascular anomalies, if the persistent primitive artery is present, it can be an access route for mechanical thrombectomy for acute ischemic stroke.
Keyword
MeSH Terms
-
Aged
Arteries*
Basilar Artery*
Carotid Artery, Internal
Cerebral Angiography
Cerebrum
Consciousness
Humans
Infarction
Magnetic Resonance Angiography
Magnetic Resonance Imaging
Middle Cerebral Artery
Quadriplegia
Stroke*
Thrombectomy
Tissue Plasminogen Activator
Unconsciousness
Urokinase-Type Plasminogen Activator
Vertebral Artery
Tissue Plasminogen Activator
Urokinase-Type Plasminogen Activator
Figure
-
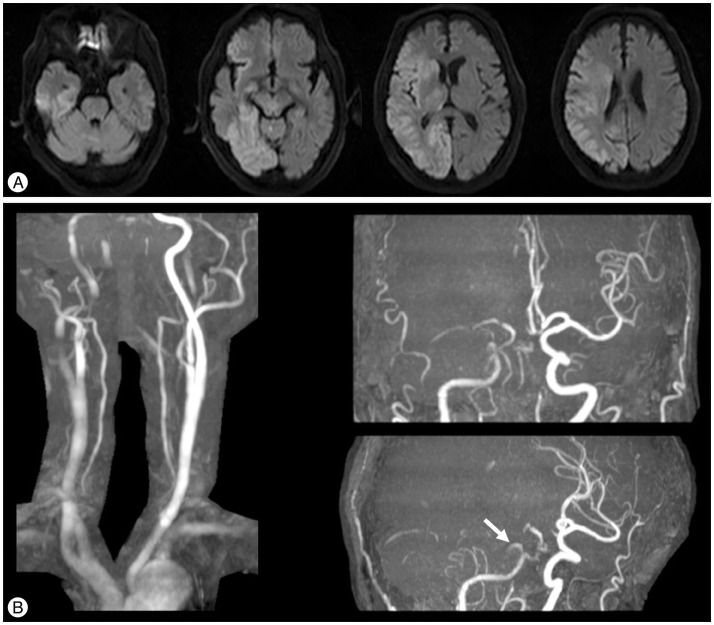
Fig. 1 A: Magnetic resonance diffusion-weighted imaging on admission showing an extensive acute infarction in the right cerebral hemisphere. B: Magnetic resonance angiography on admission showing occlusion of the right middle cerebral artery and basilar artery (BA). Bilateral extra-cranial vertebral arteries are comparatively well visualized, but bilateral intracranial VAs and the BA are poorly visualized. An unusual branch arising from the precavernous portion of the right internal carotid artery can be seen (white arrow).
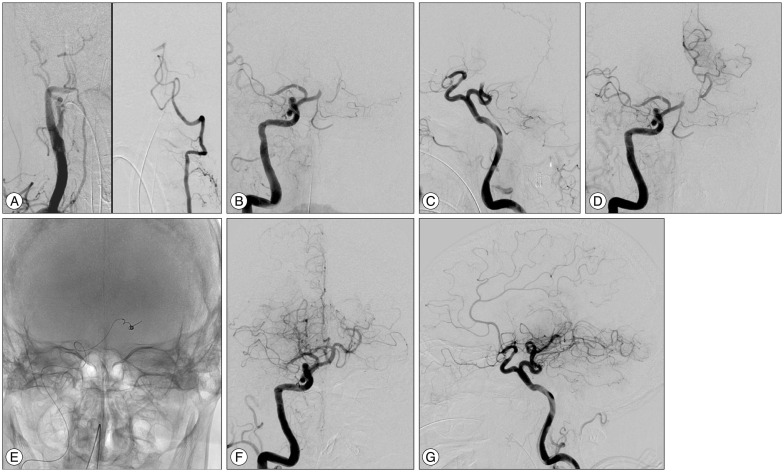
Fig. 2 A: Right innominate angiography showing a relatively hypoplastic right VA (left). Left vertebral angiography showing occlusion of the BA (right). The intracranial left VA is relatively hypoplastic. B and C: Right carotid angiography showing the occluded right middle cerebral artery and a persistent primitive trigeminal artery arising from the precavernous portion of the right internal carotid artery. D: Simultaneous angiography from the guiding catheter and the microcatheter indicating the location of the clot. E: Radioscopic image showing the Merci Retriever inserted into the left posterior cerebral artery. F and G: Final angiography after the endovascular treatment showing recanalization of the BA. VA: vertebral artery, BA: basilar artery.

Fig. 3 A: Magnetic resonance DWI at 24 hours after treatment showing new, relatively small infarctions in the left occipital lobe, left thalamus, and midbrain compared with DWI on admission. B: MRA after treatment showing good patency of the BA after the endovascular revascularization. DWI: diffusion-weighted imaging, BA: basilar artery.
Reference
-
1. Foerch C, Berkefeld J, Halbsguth A, Ziemann U, Neumann-Haefelin T. Brain stem infarction caused by proximal internal carotid artery stenosis in a patient with a persisting primitive trigeminal artery. Cerebrovasc Dis. 2006; 22:200–202. PMID: 16766871.
Article2. Fuse T, Niwa Y, Harada S. Local intraarterial fibrinolytic therapy for embolic stroke associated with vascular anomalies--two case reports. Neurol Med Chir (Tokyo). 2000; 40:641–644. PMID: 11153196.
Article3. Gasecki AP, Fox AJ, Lebrun LH, Daneault N. Bilateral occipital infarctions associated with carotid stenosis in a patient with persistent trigeminal artery. The Collaborators of the North American Carotid Endarterectomy Trial (NASCET). Stroke. 1994; 25:1520–1523. PMID: 8023373.
Article4. Gaughen JR, Starke RM, Durst CR, Evans AJ, Jensen ME. Persistent trigeminal artery : in situ thrombosis and associated perforating vessel infarction. J Clin Neurosci. 2014; 21:1075–1077. PMID: 24351576.
Article5. Iancu D, Anxionnat R, Bracard S. Brainstem infarction in a patient with internal carotid dissection and persistent trigeminal artery : a case report. BMC Med Imaging. 2010; 10:14. PMID: 20598138.6. Ikushima I, Arikawa S, Korogi Y, Uehara H, Komohara Y, Takahashi M. Basilar artery aneurysm treated with coil embolization via persistent primitive trigeminal artery. Cardiovasc Intervent Radiol. 2002; 25:70–71. PMID: 11907779.
Article7. Ito Y, Watanabe H, Niwa H, Hakusui S, Ando T, Yasuda T, et al. The protective effect of a persistent trigeminal artery on brain stem infarctions : a follow-up case report. Intern Med. 1998; 37:334–337. PMID: 9617875.
Article8. Jin SC, Park H, Kwon do H, Choi CG. Direct carotid cavernous fistula of an adult-type persistent primitive trigeminal artery with multiple vascular variations. J Korean Neurosurg Soc. 2011; 49:226–228. PMID: 21607181.
Article9. Khodadad G. Trigeminal artery and occlusive cerebrovascular disease. Stroke. 1977; 8:177–181. PMID: 847781.
Article10. Lewis VL, Cail WS. Persistent trigeminal artery with internal carotid artery occlusion. Neurosurgery. 1983; 13:314–315. PMID: 6621844.
Article11. Lin R, Vora N, Zaidi S, Aleu A, Jankowitz B, Thomas A, et al. Mechanical approaches combined with intra-arterial pharmacological therapy are associated with higher recanalization rates than either intervention alone in revascularization of acute carotid terminus occlusion. Stroke. 2009; 40:2092–2097. PMID: 19390066.
Article12. Lindsberg PJ, Mattle HP. Therapy of basilar artery occlusion : a systematic analysis comparing intra-arterial and intravenous thrombolysis. Stroke. 2006; 37:922–928. PMID: 16439705.13. Lindsberg PJ, Sairanen T, Strbian D, Kaste M. Current treatment of basilar artery occlusion. Ann N Y Acad Sci. 2012; 1268:35–44. PMID: 22994219.
Article14. Liu W, Kung DK, Mahaney KB, Rossen JD, Jabbour PM, Hasan DM. Anterior-to-posterior circulation approach for mechanical thrombectomy of an acutely occluded basilar artery using the penumbra aspiration system. World Neurosurg. 2012; 77:398.E17–398.E20. PMID: 22120391.
Article15. Loh Y, Jahan R, McArthur DL, Shi ZS, Gonzalez NR, Duckwiler GR, et al. Recanalization rates decrease with increasing thrombectomy attempts. AJNR Am J Neuroradiol. 2010; 31:935–939. PMID: 20075091.
Article16. Ogawa A, Mori E, Minematsu K, Taki W, Takahashi A, Nemoto S, et al. Randomized trial of intraarterial infusion of urokinase within 6 hours of middle cerebral artery stroke : the middle cerebral artery embolism local fibrinolytic intervention trial (MELT) Japan. Stroke. 2007; 38:2633–2639. PMID: 17702958.
Article17. Okada Y, Shima T, Nishida M, Yamada T, Yamane K, Okita S, et al. Bilateral persistent trigeminal arteries presenting with brain-stem infarction. Neuroradiology. 1992; 34:283–286. PMID: 1528434.
Article18. Sannegowda RB, Srivastava T, Jain RS, Mathur T, Jain R. Brainstem transient ischemic attacks due to compression of pons from a persistent primitive trigeminal artery. Neurol India. 2013; 61:321–322. PMID: 23860165.
Article19. Schlamann M, Doerfler A, Schoch B, Forsting M, Wanke I. Balloon-assisted coil embolization of a posterior cerebral artery aneurysm via a persistent primitive trigeminal artery : technical note. Neuroradiology. 2006; 48:931–934. PMID: 16988821.
Article20. Schwartz NE, Albers GW. Acute strokes in the setting of a persistent primitive trigeminal artery. BMJ Case Rep. 2009; 2009:bcr2006111773.
Article21. Suzuki S, Chang GY. A case of primitive trigeminal artery infarction. Neurology. 2010; 75(18 Suppl 1):S66. PMID: 21041776.
Article22. Vasović L, Jovanović I, Ugrenović S, Vlajković S, Jovanović P, Stojanović V. Trigeminal artery : a review of normal and pathological features. Childs Nerv Syst. 2012; 28:33–46. PMID: 22071960.
Article23. Waller FT, Simons RL, Kerber C, Kiesel IO, Tanabe CT. Trigeminal artery and microemboli to the brain stem. Report of two cases. J Neurosurg. 1977; 46:104–106. PMID: 556624.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of primitive persistent hypoglossal artery
- Intravenous Versus Intra-arterial Thrombolysis for Acute Ischemic Stroke Secondary to Basilar Artery Occlusion
- Endovascular Revascularization Therapy in a Patient with Acute Ischemic Stroke due to Intracranial Multiple Large-vessel Occlusion
- A Case bilateral Persistent Primitive Trigeminal Artery Combined with Cerebral Rete Mirabile
- Acute Basilar Artery Tip Thrombosis Presenting as Basilar-Subclavian Steal Phenomenon on Transcranial Doppler
