Korean J Urol.
2009 Sep;50(9):865-869.
Initial Clinical Experience with Robot-Assisted Laparoscopic Partial Nephrectomy for Complex Renal Tumors
- Affiliations
-
- 1Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea. khrha@yuhs.ac
Abstract
- PURPOSE
Robot-assisted laparoscopic partial nephrectomy (RLPN) is gaining acceptance as an alternative to open partial nephrectomy and laparoscopic partial nephrectomy for small renal masses. However, it still remains a technically challenging procedure even for experienced laparoscopists. Endophytic tumors or renal hilar tumors pose an additional challenge. MATERIALS AND METHODS: We reviewed the medical records of 11 patients (mean age: 49.3 years; range: 31-67 years) who underwent RLPN for small, complex renal masses including hilar tumors and endophytic tumors. RLPN was performed with the Da Vinci(R) surgical system (Intuitive Surgical, Sunnyvale, USA) with three robot arms and intraoperative ultrasonography (Tile-pro(R) System). RESULTS: RLPN was performed successfully without complications in all cases. The mean tumor size was 3.2 cm (range, 1.1-8.0 cm). The mean operative time was 177 minutes (range, 150-260 minutes), and the mean warm ischemia time was 32 minutes (range, 25-41 minutes). The mean estimated blood loss was 177 ml (range, 50-350 ml), and the mean hospital stay was 4 days (range, 3-7 days). Pathology found four patients with clear cell type renal cell carcinoma, one with multilocular multicystic renal cell carcinoma, two with papillary type, one with chromophobe type, and three with angiomyolipoma. CONCLUSIONS: RLPN is a feasible and safe surgery for complex renal tumors. In our experiences, RLPN could be a nephron-sparing surgical option for patients with compromised renal function and it could be an alternative to open partial nephrectomy and laparoscopic partial nephrectomy for a select group of patients.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Large posterior renal hilar tumor demonstrating proximity to renal hilar vessels and abutting the renal pelvis. CT demonstrates left 3.5 cm solid upper pole renal mass. (B) Small lateral endophytic tumor. CT demonstrates left 2 cm solid midportion renal mass.
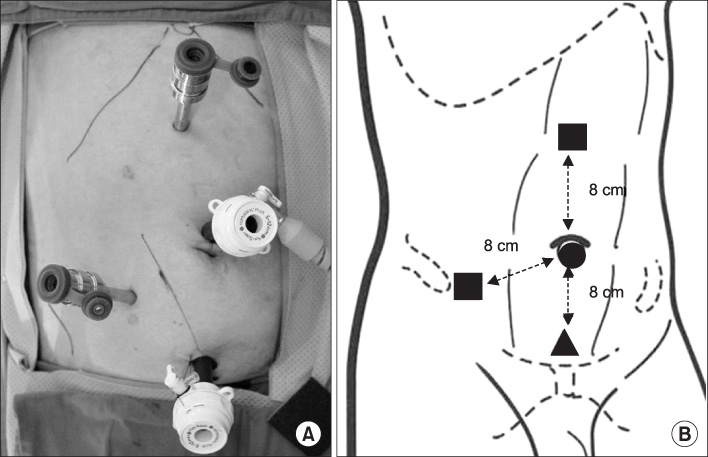
Fig. 2 (A) Port site placement for left robotic partial nephrectomy. (B) Schematic of port site placement demonstrating a 12 mm periumbilical camera port (round), two 8 mm robotic instrument ports (square), and a 12 mm assistant port.
Reference
-
1. Kaul S, Laungani R, Sarle R, Stricker H, Peabody J, Littleton R, et al. da Vinci-assisted robotic partial nephrectomy: technique and results at a mean of 15 months of follow-up. Eur Urol. 2007. 51:186–191.2. Wang AJ, Bhayani SB. Robotic partial nephrectomy versus laparoscopic partial nephrectomy for renal cell carcinoma: single-surgeon analysis of >100 consecutive procedures. Urology. 2009. 73:306–310.3. Kim KY, Kim DK, Woo SH, Kim ET, Lee SB. Laparoscopic partial nephrectomy: an useful method of decision making for determining the approach and surgical method based on the systematic classification of tumor location. Korean J Urol. 2008. 49:1067–1073.4. Park SY, Kim HJ, Seo JW, Cho KS, Ham WS, Rha KH. Robot-assisted laparoscopic partial nephrectomy. Korean J Urol. 2008. 49:387–391.5. Gettman MT, Blute ML, Chow GK, Neururer R, Bartsch G, Peschel R. Robotic-assisted laparoscopic partial nephrectomy: technique and initial clinical experience with DaVinci robotic system. Urology. 2004. 64:914–918.6. Phillips CK, Taneja SS, Stifelman MD. Robot-assisted laparoscopic partial nephrectomy: the NYU technique. J Endourol. 2005. 19:441–445.7. Stifelman MD, Caruso RP, Nieder AM, Taneja SS. Robot-assisted laparoscopic partial nephrectomy. JSLS. 2005. 9:83–86.8. Caruso RP, Phillips CK, Kau E, Taneja SS, Stifelman MD. Robot assisted laparoscopic partial nephrectomy: initial experience. J Urol. 2006. 176:36–39.9. Rogers CG, Metwalli A, Blatt AM, Bratslavsky G, Menon M, Linehan WM, et al. Robotic partial nephrectomy for renal hilar tumors: a multi-institutional analysis. J Urol. 2008. 180:2353–2356.10. Deane LA, Lee HJ, Box GN, Melamud O, Yee DS, Abraham JB, et al. Robotic versus standard laparoscopic partial/wedge nephrectomy: a comparison of intraoperative and perioperative results from a single institution. J Endourol. 2008. 22:947–952.11. Allaf ME, Bhayani SB, Rogers C, Varkarakis I, Link RE, Inagaki T, et al. Laparoscopic partial nephrectomy: evaluation of long-term oncological outcome. J Urol. 2004. 172:871–873.12. Lane BR, Gill IS. 5-year outcomes of laparoscopic partial nephrectomy. J Urol. 2007. 177:70–74.13. Aron M, Koenig P, Kaouk JH, Nguyen MM, Desai MM, Gill IS. Robotic and laparoscopic partial nephrectomy: a matched-pair comparison from a high-volume centre. BJU Int. 2008. 102:86–92.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robotic Radical Nephrectomy with Vena Caval Tumor Thrombectomy: Experience of Novice Robotic Surgeons
- How far has robot-assisted partial nephrectomy reached?
- Current Status of Partial Nephrectomy for Renal Mass
- Laparoscopic Partial Nephrectomy using a Microwave Tissue Coagulator for Small Renal Tumor
- Initial Clinical Experience of Simultaneous Robot-Assisted Bilateral Partial Nephrectomy and Radical Prostatectomy
