Vertical distance between umbilicus to aortic bifurcation on coronal view in Korean women
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Seoul National University Hospital, Seoul, Korea.
- 2Department of Obstetrics and Gynecology, Seoul National University Bundang Hospital, Seongnam, Korea. blasto@snubh.org
- 3Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Korea.
Abstract
OBJECTIVE
To evaluate the vertical distance between umbilicus to aortic bifurcation on coronal view in Korean women and their relation with body mass index (BMI) and woman's age.
METHODS
This retrospective study included 257 women who visited emergency center at university-based hospital from January to December 2011. All women underwent abdomino-pelvic computerized tomography (CT) due to various symptoms in a supine position. By using the electronic coronal CT images, the vertical distance between umbilicus and aortic bifurcation was measured. If aortic bifurcation was located below umbilicus, the distance was expressed as minus value (i.e., caudal to umbilicus). Age of woman, body weight, height and calculated BMI (kg/m2) were also recorded.
RESULTS
Aortic bifurcation was located caudal to umbilicus in 52.9% and cephalad to umbilicus in 37.4%. The vertical distance had a negative relationship with BMI (r=.0.180, P=0.004), as well as woman's age (r=-0.382, P<0.001). However, a multivariate analysis revealed that the vertical distance had a significant negative relationship with woman's age (P<0.001) but not with BMI (P=0.510). An equation could be drawn to estimate the vertical distance by using woman's age and BMI: vertical distance (mm)=12.6-0.3x(age)-0.2x(BMI).
CONCLUSION
The vertical distance from umbilicus to aortic bifurcation on coronal view showed a significant inverse correlation with woman's age, however, the distances varied widely. Most older or obese Korean women had aortic bifurcation caudal to umbilicus.
MeSH Terms
Figure
-
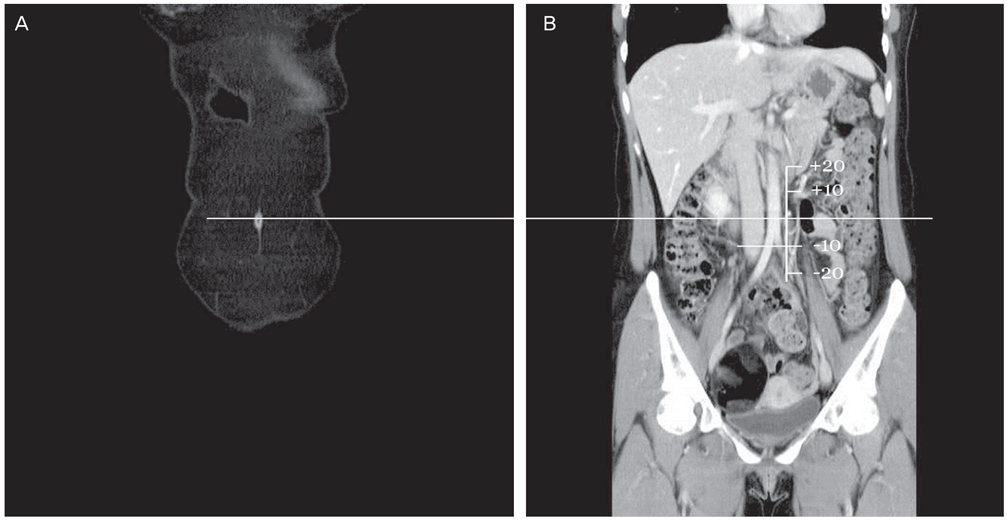
Fig. 1 Method to measure the vertical distance between the umbilicus and aortic bifurcation by using the electronic coronal computed tomography images. After marking the center of the umbilicus (A), consecutive images are tracking until aortic bifurcation appears (B), and then the distance from the extension line of umbilicus and aortic bifurcation is measured as unit of millimeter. If aortic bifurcation is located below umbilicus, the distance is expressed as minus value. Approximately 5 cm sized mature cystic teratoma is seen on right ovary in this woman, but this case is included because relatively small tumor within pelvis does not cause dislocation of umbilicus and/or aortic bifurcation.
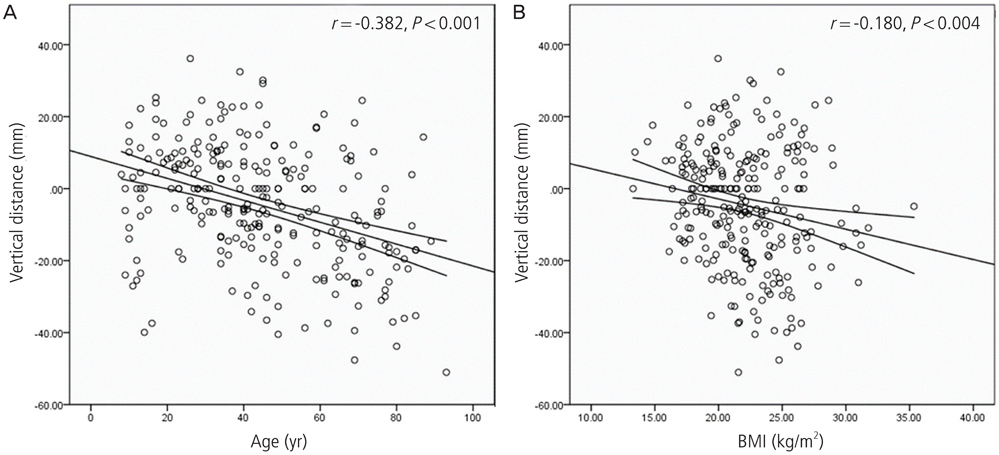
Fig. 2 A linear regression line to show a negative correlation between vertical distance (umbilicus-to-aortic bifurcation) and woman's age (A) or body mass index (BMI) (B). The minus values indicate that aortic bifurcation located caudally to umbilicus.
Reference
-
1. Nezhat F, Brill AI, Nezhat CH, Nezhat A, Seidman DS, Nezhat C. Laparoscopic appraisal of the anatomic relationship of the umbilicus to the aortic bifurcation. J Am Assoc Gynecol Laparosc. 1998; 5:135–140.2. Chapron CM, Pierre F, Lacroix S, Querleu D, Lansac J, Dubuisson JB. Major vascular injuries during gynecologic laparoscopy. J Am Coll Surg. 1997; 185:461–465.3. Fruhwirth J, Koch G, Mischinger HJ, Werkgartner G, Tesch NP. Vascular complications in minimally invasive surgery. Surg Laparosc Endosc. 1997; 7:251–254.4. Lafullarde T, Van Hee R, Gys T. A safe and simple method for routine open access in laparoscopic procedures. Surg Endosc. 1999; 13:769–772.5. Schafer M, Lauper M, Krahenbuhl L. A nation's experience of bleeding complications during laparoscopy. Am J Surg. 2000; 180:73–77.6. Tsai CC, Semmens JP, Semmens EC, Lam CF, Lee FS. Vaginal physiology in postmenopausal women: pH value, transvaginal electropotential difference, and estimated blood flow. South Med J. 1987; 80:987–990.7. Dwyer JH, Lippert P, Rieger-Ndakorerwa GE, Semmer NK. Centers for Disease Control (CDC). Some chronic disease risk factors and cigarette smoking in adolescents: the Berlin-Bremen Study. MMWR Morb Mortal Wkly Rep. 1987; 36:Suppl 4. 35S–40S.8. Semm K, Mettler L, Michelmann HW. The effect of bacterial contamination on pregnancy rate after in vitro fertilization (IVF) and embryo transfer (ET) in humans. Dtsch Tierarztl Wochenschr. 1987; 94:503–506.9. Kurzel RB, Edinger DD Jr. Injury to the great vessels: a hazard of transabdominal endoscopy. South Med J. 1983; 76:656–657.10. Sriprasad S, Yu DF, Muir GH, Poulsen J, Sidhu PS. Positional anatomy of vessels that may be damaged at laparoscopy: new access criteria based on CT and ultrasonography to avoid vascular injury. J Endourol. 2006; 20:498–503.11. Schuhmacher JH, Clorius JH, Semmler W, Hauser H, Matys ER, Maier-Borst W, et al. NMR relaxation times T1 and T2 of water in plasma from patients with lung carcinoma: correlation of T2 with blood sedimentation rate. Magn Reson Med. 1987; 5:537–547.12. Al-Talib A, Alharbi F, Valenti D, Tulandi T. Location of aortic bifurcation and transverse colon in postmenopausal women: relevance to laparoscopy. Surg Technol Int. 2010; 19:130–134.13. Poindexter AN, Ritter M, Fahim A, Humphrey H. Trocar introduction performed during laparoscopy of the obese patient. Surg Gynecol Obstet. 1987; 165:57–59.14. Hurd WH, Bude RO, DeLancey JO, Gauvin JM, Aisen AM. Abdominal wall characterization with magnetic resonance imaging and computed tomography. The effect of obesity on the laparoscopic approach. J Reprod Med. 1991; 36:473–476.15. Semmel H. Towards a national health program. National health is back on the agenda. Health PAC Bull. 1987; 17:4–7.16. Cravello L, D'Ercole C, Roger V, Samson D, Blanc B. Laparoscopic surgery in gynecology: randomized prospective study comparing pneumoperitoneum and abdominal wall suspension. Eur J Obstet Gynecol Reprod Biol. 1999; 83:9–14.17. Larobina M, Nottle P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg Laparosc Endosc Percutan Tech. 2005; 15:119–123.18. Penfield AJ. How to prevent complications of open laparoscopy. J Reprod Med. 1985; 30:660–663.19. Deffieux X, Ballester M, Collinet P, Fauconnier A, Pierre F. French National College of Gynaecologists and Obstetricians. Risks associated with laparoscopic entry: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians. Eur J Obstet Gynecol Reprod Biol. 2011; 158:159–166.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiologic Localization and Lengths of Umbilical Artery Catheter to Major Aortic Branches Determined by Ultrasonography in Neonates
- Multi-Detector Computed Tomography Coronal View for Deciding Optimal Incision Site in Acute Appendicitis
- Umbilical Shape and Diseases Related to Age and Sex
- Fluoroscopic Landmark to Optimize the View of the Foramen Ovale Using the Neighboring Structure
- Location of the umbilicus in Korean women and its changes after breast reconstruction with an ipsilateral pedicled rectus abdominis musculocutaneous flap
