Korean J Urol.
2009 Feb;50(2):135-139.
A Short-Term Analysis of Parameters Affecting the Outcome of Sacral Neuromodulation
- Affiliations
-
- 1Department of Urology, Ewha Womans University School of Medicine, Seoul, Korea. wowhana@ewha.ac.kr
Abstract
- PURPOSE
Sacral neuromodulation has become an effective option for controlling intractable symptoms of overactive bladder: urgency and urge incontinence. However, it has its limitations in that an intermittent pulse generator (IPG) is insertable only in patients with symptom improvement of at least 50%. In this study, we aimed to investigate the parameters that predict surgical outcomes.
MATERIALS AND METHODS
Data from 31 candidates for sacral neuromodulation were retrospectively analyzed. Twenty patients out of 31 candidates had satisfactory symptom improvement after tinned lead test implantation, which resulted in IPG implantation. Data and neural stimulation parameters were compared and analyzed between successful IPG implants (group 1) and test failures (group 2).
RESULTS
The percentage of female patients was higher in the IPG implant group (group 1: 95%, group 2: 64%). There was a significant difference in symptom duration, between the two groups (group 1: 40.5 months, group 2: 91 months). There was a significant difference in the number of episodes of urgency between the two groups (group 1: 6.83/day, group 2: 9.66/day, p=0.012), and severity of urgency showed significant difference between two groups (group 1CONCLUSIONS
In females, the severity and duration of symptoms may be factors predicting poor response to neuromodulation. Although there is a need for further data analysis, this study suggests that the proper selection of surgical time is important in controlling patients' lower urinary tract symptoms by neuromodulation.
Keyword
MeSH Terms
Figure
-
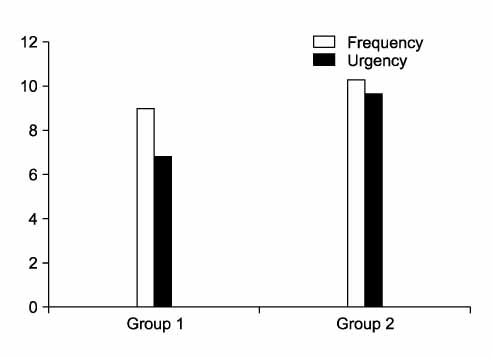
Fig. 1 Differences in frequency (p=0.684) and urgency (p=0.012) between group 1 (IPG insertion) and group 2 (IPG insertion fail). IPG: intermittent pulse generator.
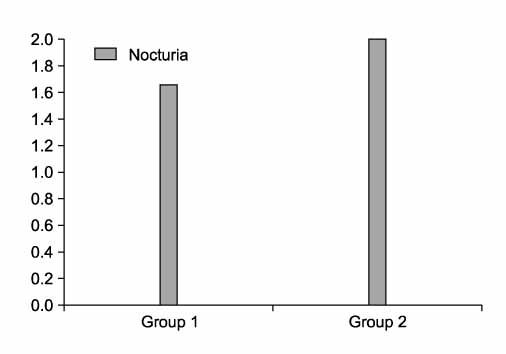
Fig. 2 Differences in nocturia (p=0.454) between group 1 (IPG insertion) and group 2 (IPG insertion fail). IPG: intermittent pulse generator.
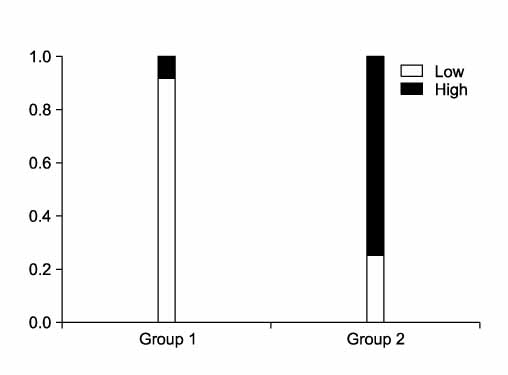
Fig. 3 Differences in intensity of urgency (p=0.027) between group 1 (IPG insertion) and group 2 (IPG insertion fail). IPG: intermittent pulse generator.
Reference
-
1. Wein AJ. Diagnosis and treatment of the overactive bladder. Urology. 2003. 62:5 Suppl 2. 20–27.2. Spinelli M, Bertapelle P, Cappellano F, Zanollo A, Carone R, Catanzaro F, et al. Chronic sacral neuromodulation in patients with lower urinary tract symptoms: results from a national register. J Urol. 2001. 166:541–545.3. van Kerrebroeck PE, van Voskuilen AC, Heesakkers JP, Lycklama á Nijholt AA, Siegel S, Jonas U, et al. Results of sacral neuromodulation therapy for urinary voiding dysfunction: outcomes of a prospective, worldwide clinical study. J Urol. 2007. 178:2029–2034.4. Leng WW, Morrisroe SN. Sacral nerve stimulation for the overactive bladder. Urol Clin North Am. 2006. 33:491–501.5. Hassouna MM, Elkelini MS. Early versus late treatment of voiding dysfunction with pelvic neuromodulation. Can Urol Assoc J. 2007. 1:106–110.6. Chartier-Kastler EJ, Ruud Bosch JL, Perrigot M, Chancellor MB, Richard F, Denys P. Long-term results of sacral nerve stimulation (S3) for the treatment of neurogenic refractory urge incontinence related to detrusor hyperreflexia. J Urol. 2000. 164:1476–1480.7. Chai TC. Surgical techniques of sacral implantation. Urol Clin North Am. 2005. 32:27–35.8. Brown JS, Vittinghoff E, Wyman JF, Stone KL, Nevitt MC, Ensrud KE, et al. Urinary incontinence: Does it increase risk for falls and fractures? Study of Osteoporotic Fractures Research Group. J Am Geriatr Soc. 2000. 48:721–725.9. Zorn BH, Montgomery H, Pieper K, Gray M, Steers WD. Urinary incontinence and depression. J Urol. 1999. 162:82–84.10. Stewart WF, Van Rooyen JB, Cundiff GW, Abrams P, Herzog AR, Corey R, et al. Prevalence and burden of overactive bladder in the United States. World J Urol. 2003. 20:327–336.11. Lee KS, Lee YS. Overactive bladder. Korean J Urol. 2007. 48:1191–1208.12. Ouslander JG. Management of overactive bladder. N Engl J Med. 2004. 350:786–799.13. Yoo JS, Kim JC, Hwang TK. Predictors of antimuscarinic treatment response for female patients with overactive bladder. Korean J Urol. 2007. 48:66–71.14. Bernstein AJ, Peters KM. Expanding indications for neuromodulation. Urol Clin North Am. 2005. 32:59–63.15. Aboseif S, Tamaddon K, Chalfin S, Freedman S, Kaptein J. Sacral neuromodulation as an effective treatment for refractory pelvic floor dysfunction. Urology. 2002. 60:52–56.16. Bradley WE, Timm GW, Chou SN. A decade of experience with electronic stimulation of the micturition reflex. Urol Int. 1971. 26:283–302.17. Juenemann KP, Lue TF, Schmidt RA, Tanagho EA. Clinical significance of sacral and pudendal nerve anatomy. J Urol. 1988. 139:74–80.18. Tanagho EA, Schmidt RA, de Araujo CG. Urinary striated sphincter: What is its nerve supply? Urology. 1982. 20:415–417.19. Lukban JC, Whitmore KE, Sant GR. Current management of interstitial cystitis. Urol Clin North Am. 2002. 29:649–660.20. Everaert K, Devulder J, Dee Muynck M, Stockman S, Depaepe H, Dee Looze D, et al. The pain cycle: implications for the diagnosis and treatment of pelvic pain syndromes. Int Urogynecol J Pelvic Floor Dysfunct. 2001. 12:9–14.21. Siegel S, Paszkiewicz E, Kirkpatrick C, Hinkel B, Oleson K. Sacral nerve stimulation in patients with chronic intractable pelvic pain. J Urol. 2001. 166:1742–1745.22. Comiter CV. Sacral neuromodulation for the symptomatic treatment of refractory interstial cystitis: a prospective study. J Urol. 2003. 169:1369–1373.23. Peters KM, Konstandt D. Sacral neuromodulation decreases narcotic requirements in refractory interstitial cystitis. BJU Int. 2004. 93:777–779.24. Peters KM, Carey JM, Konstandt DB. Sacral neuromodulation for the treatment of refractory interstitial cystitis: outcomes based on technique. Int Urogynecol J Pelvic Floor Dysfunction. 2003. 14:223–228.25. Chung JW, Han DH, Lee KS. Efficacy and safety of sacral neuromodulation (Interstim®.) for the treatment of refractory overactive bladder symptoms and chronic pelvic pain. Korean J Urol. 2007. 48:701–705.26. Groenendijk PM, Heesakkers JP, Lycklama A, Nijeholt AA. Urethral instability and sacral nerve stimulation-a better parameter to predict efficacy? J Urol. 2007. 178:568–572.27. Cohen BL, Tunuguntla HS, Gousse A. Predictors of success for first stage neuromodulation: motor versus sensory response. J Urol. 2006. 175:2178–2180.28. Malaguti S, Spinelli M, Giardiello G, Lazzeri M, Van Den Hombergh U. Neurophysiological evidence may predict the outcome of sacral neuromodulation. J Urol. 2003. 170:2323–2326.29. Goh M, Diokno AC. Sacral neuromodulation for nonobstructive urinary retention- Is success predictable? J Urol. 2007. 178:197–199.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiographic Position of the Electrode as a Predictor of the Outcome of InterStim Therapy
- Sacral Neuromodulation in Patients With a Cardiac Pacemaker
- Needle Placement: A Guide to Predictable Sensory and Motor Responses Based on Variations in Needle Placement During Sacral Neuromodulation Procedures
- Sleep disturbance changes in women after treatment of refractory overactive bladder with sacral neuromodulation
- Neuromodulation for Insomnia Management
