Korean Circ J.
2011 May;41(5):276-279. 10.4070/kcj.2011.41.5.276.
Progressive Familial Heart Block Type I in a Korean Patient
- Affiliations
-
- 1Division of Cardiology, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea. drshin@mail.ulsan.ac.kr
- 2Division of Cardiology, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2297936
- DOI: http://doi.org/10.4070/kcj.2011.41.5.276
Abstract
- A 29-year-old man was referred to the emergency department with a complaint of abdominal pain and dizziness. He had experienced two previous syncopal episodes. His family history revealed that his mother and his two uncles had received permanent pacemaker implantation. His initial heart rate was 49 beats per minute. The electrocardiography (ECG) showed atrial flutter and right bundle branch block (RBBB) with left anterior fascicular block (LAFB). On admission, 24-hour Holter showed ventricular pause up to 16 seconds during syncope. Radio frequency catheter ablation (RFCA) of atrial flutter was performed. The ECG revealed bifascicular block (RBBB and LAFB) and first-degree atrioventricular block. He received a permanent pacemaker implantation. His brother's and his sister's ECGs also showed trifascicular block and the pedigree showed autosomal dominant inheritance. This patient was diagnosed with a progressive familial heart block (PFHB) type I. This would be the first report of a PFHB type I case documented in Korea.
MeSH Terms
Figure
-

Fig. 1 Initial ECG shows atrial flutter with bifascicular block; RBBB and LAFB (A). Twenty four-hour Holter shows asystole up to 16 seconds (B). ECG after RFCA shows trifascicular block; first-degree atrioventricular block, RBBB and LAFB (C). The patient received a permanent pacemaker implantation (D). ECG: electrocardiography, RBBB: right bundle branch block, LAFB: left anterior fascicular block.
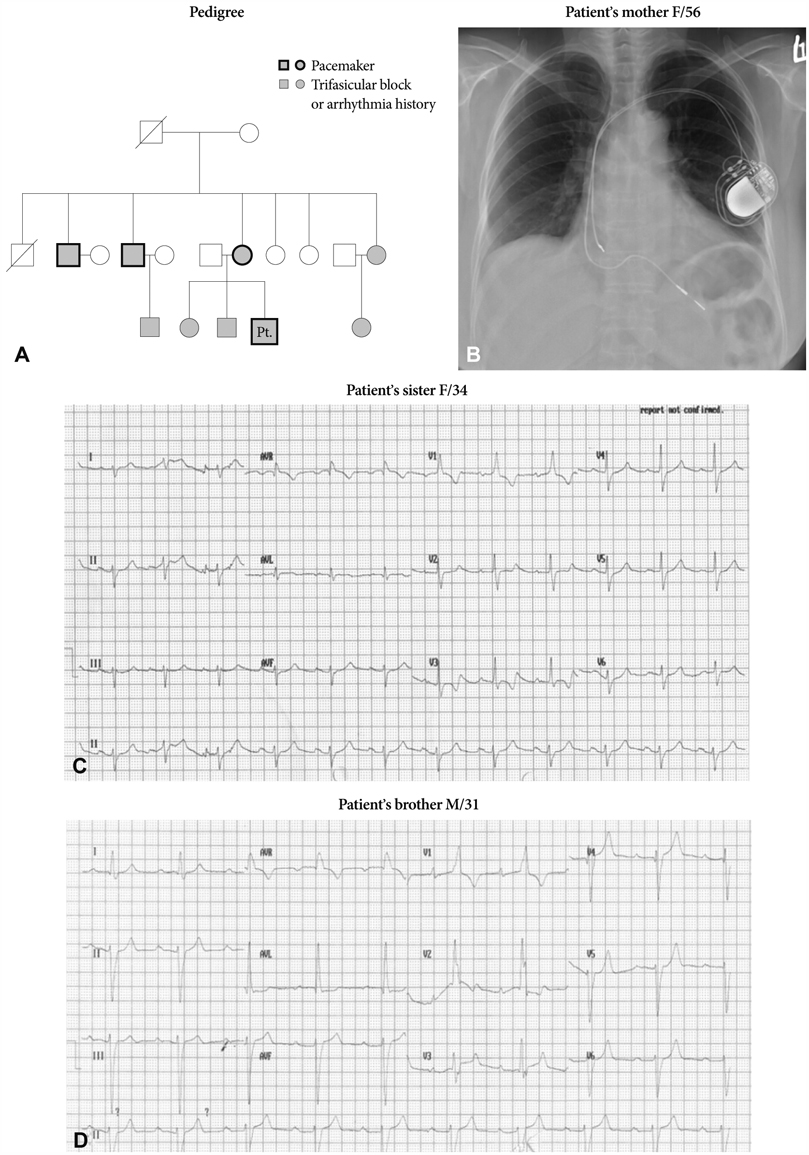
Fig. 2 The pedigree showed an autosomal dominant inheritance (A). The patient's mother received a permanent pacemaker implantation at the age of 51 years (B). His brother's and his sister's electrocardiography also showed trifascicular block (C and D). Pt.: patient.
Reference
-
1. Brink AJ, Torrington M. Progressive familial heart block: two types. S Afr Med J. 1977. 52:53–59.2. van der Merwe PL, Weymar HW, Torrinton M, Brink AJ. Progressive familial heart block: part II. clinical and ECG confirmation of progression-report on 4 cases. S Afr Med J. 1986. 70:356–357.3. Brink PA, Ferreira A, Moolman JC, Weymar HW, van der Merwe PL, Corfield VA. Gene for progressive familial heart block type I maps to chromosome 19q13. Circulation. 1995. 91:1633–1640.4. Bardien-Kruger S, Wulff H, Arieff Z, Brink P, Chandy KG, Corfield V. Characterization of the human voltage-gated potassium channel gene, KCNA7, a candidate gene for inherited cardiac disorders, and its exclusion as cause of progressive familial heart block I (type I PFHB). Eur J Hum Genet. 2002. 10:36–43.5. Brink PA, Moolman-Smook JC, Corfield VA. Mendelian-inherited heart disease: a gateway to understanding mechanisms in heart disease Update on work done at the University of Stellenbosch. Cardiovasc J Afr. 2009. 20:57–63.6. Brink PA, Moolman JC, Ferreira A, et al. Genetic linkage studies of progressive familial heart block, a cardiac conduction disorder. S Afr J Sci. 1994. 90:236–240.7. van der Merwe PL, Weymar HW, Torrington M, et al. Progressive familial heart block (type I): a follow-up study after 10 years. S Afr Med J. 1988. 73:275–276.8. Kim WJ, Shim JJ, Kim HS, et al. Familial sick sinus syndrome. Korean Circ J. 2003. 33:1155–1160.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kearns-sayre Syndrome Treated with Permanent Pacemaker Insertion for Complete Atrioventricular Block
- Conduction Block in Hereditary Motor Sensory Neuropathy
- A Case Report of Anesthetic Management in a Patient with Complete Left Bundle Braneh Block
- High Grade Atrioventricular Block during Cesarean Section under General Anesthesia in a Parturient with Mobitz Type I Atrioventricular Block: A case report
- Retrograde Conduction in Complete Heart Block
