Kearns-sayre Syndrome Treated with Permanent Pacemaker Insertion for Complete Atrioventricular Block
- Affiliations
-
- 1Division of Cardiology, College of Medicine, the Catholic University of Korea, Seoul, Korea. hhhsungho@naver.com
- KMID: 2384843
- DOI: http://doi.org/10.7180/kmj.2017.32.1.133
Abstract
- Kearns-Sayre syndrome (KSS) is a rare multisystem mitochondrial disorder associated with progressive external ophthalmoplegia, atypical pigmentary degeneration of the retina, and complete heart block. KSS can lead to a risk of sudden death because of the potential progression of conduction abnormalities such as right or left bundle branch block or complete atrioventricular (AV) block. Here we describe the case of a KSS patient with type I diabetes who experienced syncope in the presence of complete AV block, confirmed by muscular biopsy.
MeSH Terms
Figure
-

Fig. 1 ECG revealed complete atrioventricular block with a wide QRS (150 ms) and ventricular rhythm of 34 beats per minute (bpm) (A), normal finding at 9 years old (B), and pacemaker rhythm(DDDR type). (C).

Fig. 2 Ophthalmoscopy of the fundus showed atypical retinal pigmentary degeneration (salt and pepper retinitis) (red arrow).
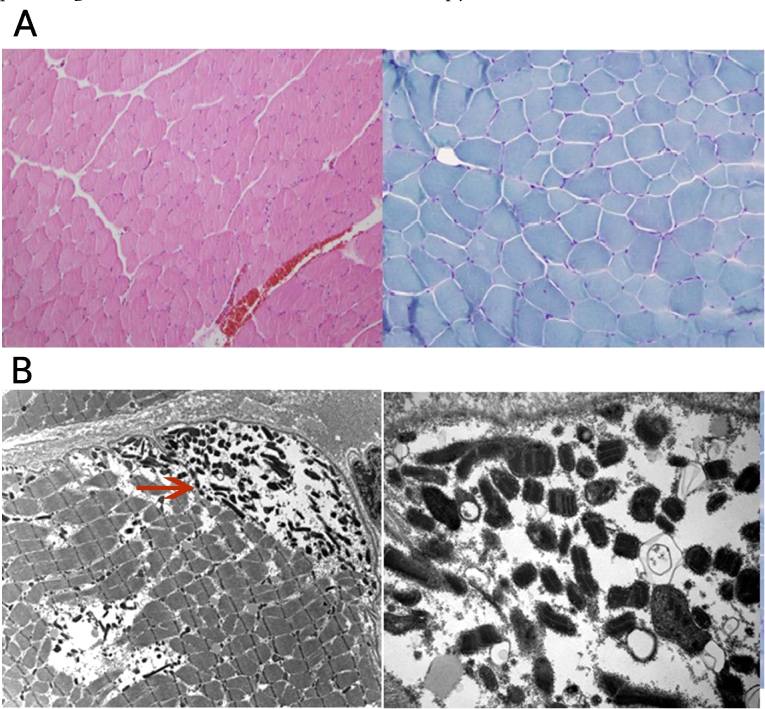
Fig. 3 Light and electron microscopic examination of the right thigh muscle Modified trichrome stain revealed no diagnostic abnormalities such as ragged red fibers, similar to other enzyme histochemical and immunohistochemical stains (A, LM finding), but showed muscle cells with subsarcolemmal collection of mitochondria, many of them containing crystalline inclusions (red arrow), electron microscopically consistent with mitochondrial myopathy (B, EM finding).
Reference
-
1. Duning T, Deppe M, Keller S, Mohammadi S, Schiffbauer H, Marziniak M. Diffusion tensor imaging in a case of Kearns-Sayre syndrome: striking brainstem involvement as a possible cause of oculomotor symptoms. J Neurol Sci. 2009; 281:110–112.
Article2. Chawla S, Coku J, Forbes T, Kannan S. Kearns-Sayre syndrome presenting as complete heart block. Pediatr Cardiol. 2008; 29:659–662.
Article3. Franzese A, Del Giudice E, Santoro L, De Filippo G, Argenziano A. Diabetes mellitus in Kearns-Sayre syndrome: a case with a 10-year follow-up. Diabetes Res Clin Pract. 1995; 30:233–235.
Article4. Riera AR, Kaiser E, Levine P, Schapachinik E, Dubner S, Ferreira C, et al. Kearns-Sayre syndrome: electro-vectorcardiographic evolution for left septal fascicular block of the his bundle. J Electrocardiol. 2008; 41:675–678.
Article5. Yorifuji S, Ogasahara S, Takahashi M, Tarui S. Decreased activities in mitochondrial inner membrane electron transport system in muscle from patients with Kearns-Sayre syndrome. J Neurol Sci. 1985; 71:65–75.
Article6. Tranchant C, Mousson B, Mohr M, Dumoulin R, Welsch M, Weess C, et al. Cardiac transplantation in an incomplete Kearns-Sayre syndrome with mitochondrial DNA deletion. Neuromuscul Disord. 1993; 3:561–566.
Article7. Puri A, Pradhan A, Chaudhary G, Singh V, Sethi R, Narain VS. Symptomatic complete heart block leading to a diagnosis of Kearns-Sayre syndrome. Indian heart J. 2012; 64:515–517.
Article8. Park IH, Lim JK, Moon JG, Joung BY, Lee MH, Kim SS. A Case of Kearns Sayre syndrome complicated with complete AV block. Korean J Med. 2006; 70:564–568.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of KearnsSayre syndrome complicated with complete AV block
- Results of Permanent Cardiac Pacemaker Implantation in Ewha Womans University Mokdong Hospital
- Clinical manifestations and anesthetic management of Kearns-Sayre syndrome: A case report
- A Case of Cardiac Amyloidosis with Complete Atrioventricular Conduction Block Treated by Permanent Pacemaker
- Kearns-Sayre Syndrome: 3 Case Reports and Review of Clinical Feature
