Malignant Pheochromocytoma that Recurred in the Contralateral Adrenal Gland and Metastasized to the Bladder
- Affiliations
-
- 1Department of Urology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. chung90@sanggyepaik.ac.kr
- 2Department of General Surgery, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 3Department of Diagnostic Radiology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 4Department of Pathology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- KMID: 2294326
- DOI: http://doi.org/10.4111/kju.2006.47.7.797
Abstract
- Pheochromocytoma is an uncommon neoplasm and it is derived from the neural crest. It is one of the surgically curable hypertensive syndromes. The sequela of this disease can be serious if definite treatment is not promptly performed. We report here on a case of malignant pheochromocytoma that recurred in the contralateral adrenal gland and it subsequently metastasized to the bladder after the patient refused treatment of the contralateral adrenal tumor.
Keyword
MeSH Terms
Figure
-

Fig. 1 Abdominal computer tomography taken 10 years before presentation shows a well-defined round mass with peripheral marked enhancement and central necrosis in the anterior portion of the left kidney (white arrowhead).
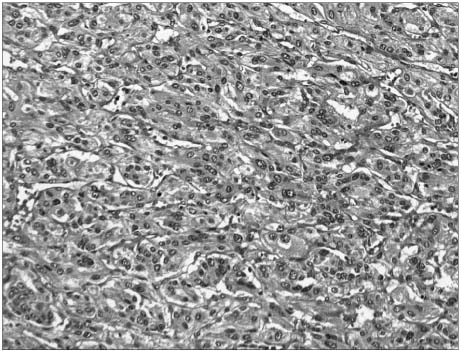
Fig. 2 Microscopic finding of the left adrenal mass lesion that is resected 10 years before. It reveals pheochromocytoma and shows a small alveolar pattern of growth with balls or cords of cells ("Zellballen") that are delimited from each other by connective tissues and vascular septations. Mitotic figures are uncommonly seen (H&E, ×150).
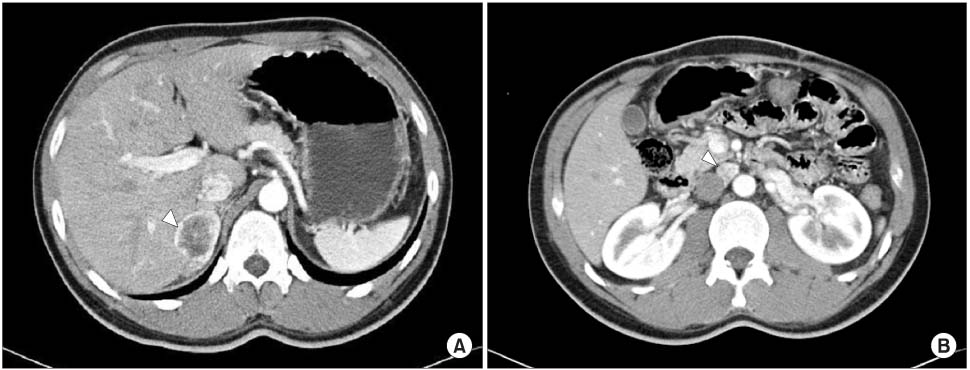
Fig. 3 Abdominal computer tomography shows recurrent mass lesion involving the right adrenal gland (7.0×4.2×2.1cm, white arrowhead) (A) and enlargement of the aorto-caval lymph node (3.5×2.1×1.5cm, white arrowhead) (B).
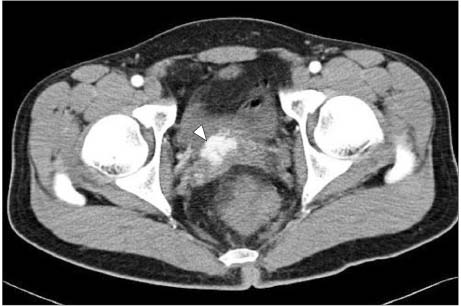
Fig. 4 Pelvic computer tomography shows well-enhancing mass lesion between the posterior wall of the bladder and the seminal vesicle (2.8×1.9×1.8cm).

Fig. 5 18F-FDG PET shows increased uptakes in the right adrenal gland (white) and the aorto-caval lymph node (black).
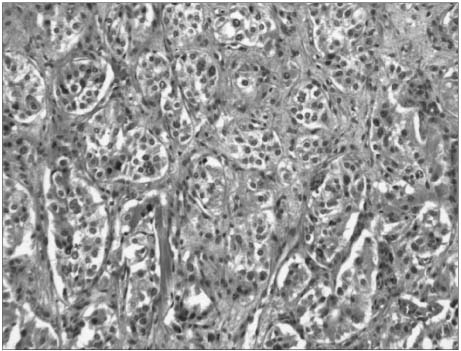
Fig. 6 Microscopic finding of the right adrenal mass shows an alveolar pattern with distinct nests of cells ("Zellballen"); this is identical to the left adrenal mass lesion that is resected 10 years before (H&E, ×200).
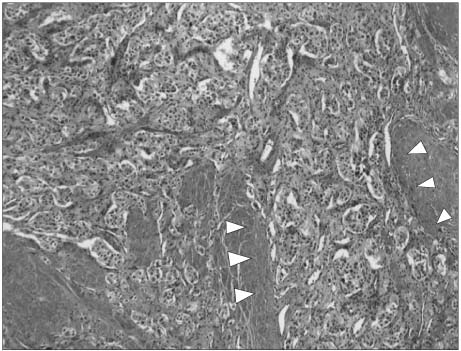
Fig. 7 Microscopic finding of the bladder mass shows the same finding as the adrenal mass. The bladder mass is located in the detrusor muscle (arrowheads) (H&E, ×100).
Reference
-
1. Goldstein RE, O'Neill JA Jr, Holcomb GW III, Morgan WM III, Neblett WW III, Oates JA, et al. Clinical experience over 48 years with pheochromocytoma. Ann Surg. 1999. 229:755–764.2. John H, Ziegler WH, Hauri D, Jaeger P. Pheochromocytomas: Can malignant potential be predicted? Urology. 1999. 53:679–683.3. Noshiro T, Shimizu K, Watanabe T, Akama H, Shibukawa S, Miura W, et al. Changes in clinical features and long-term prognosis in patients with pheochromocytoma. Am J Hypertens. 2000. 13:35–43.4. Lack EE. Lack EE, editor. Adrenal medullary hyperplasia and pheochromocytoma. Pathology of adrenal and extraadrenal paraganglia. Major problems in pathology. 1994. Philadelphia: WB Saunders;220–272.5. Thompson LD. Pheochromocytoma of the Adrenal Gland Scaled Score (PASS) to separate benign from malignant neoplasms: a clinicopathologic and immunophenotypic study of 100 cases. Am J Surg Pathol. 2002. 26:551–566.6. Stenstrom G, Svardsudd K. Pheochromocytoma in Sweden 1958-1981. An analysis of the National Cancer Registry Data. Acta Med Scand. 1986. 220:220–232.7. Padmanabhan H, Ehrlich LD, Quazedo M, Fojo T, Louie A, Walther M, et al. Unusual locations of involvement by malignancies: case 2. Metastatic pheochromocytoma to the colon. J Clin Oncol. 2003. 21:3369–3371.8. Lee YS, Oh KH. Clinical evaluation of 12 cases of pheochromocytoma. Korean J Urol. 1993. 34:619–625.9. Mamede M, Carrasquillo JA, Chen CC, Corral PD, Whatley M, Ilias I, et al. Discordant localization of 2-[18F]-fluoro-2-deoxy-D-glucose in 6-[18F]-fluorodopamine- and [123I]-metaiodobenzylguanidine-negative metastatic pheochromocytoma sites. Nucl Med Commun. 2006. 27:31–36.10. Brouwers FM, Petricoin EF 3rd, Ksinantova L, Breza J, Rajapakse V, Ross S, et al. Low molecular weight proteomic information distinguishes metastatic from benign pheochromocytoma. Endocr Relat Cancer. 2005. 12:263–272.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Malignant Pheochromocytoma
- A Case of Nonfunctioning Pheochromocytoma of the Bladder
- A Case of Adrenal Cystic Pheochromocytoma with Contralateral Adrenocortical Adenoma Causing Subclinical Cushing's Syndrome
- A Case of Pheochromocytoma
- Huge pheochromocytoma presented with paraaortic lymph node and spine metastases
